Spinal decompression and Digestion. No one wants to worry about stomach issues. A rich and unhealthy diet can cause digestive issues, stomach pain, and back pain. This can turn into a severe chronic condition; studies have found links between spinal problems and gastrointestinal tract symptoms, which include:
Abdominal pain that radiates.
Constipation.
Difficulty controlling bowel movements.
Diarrhea.
Nausea.
Vomiting.
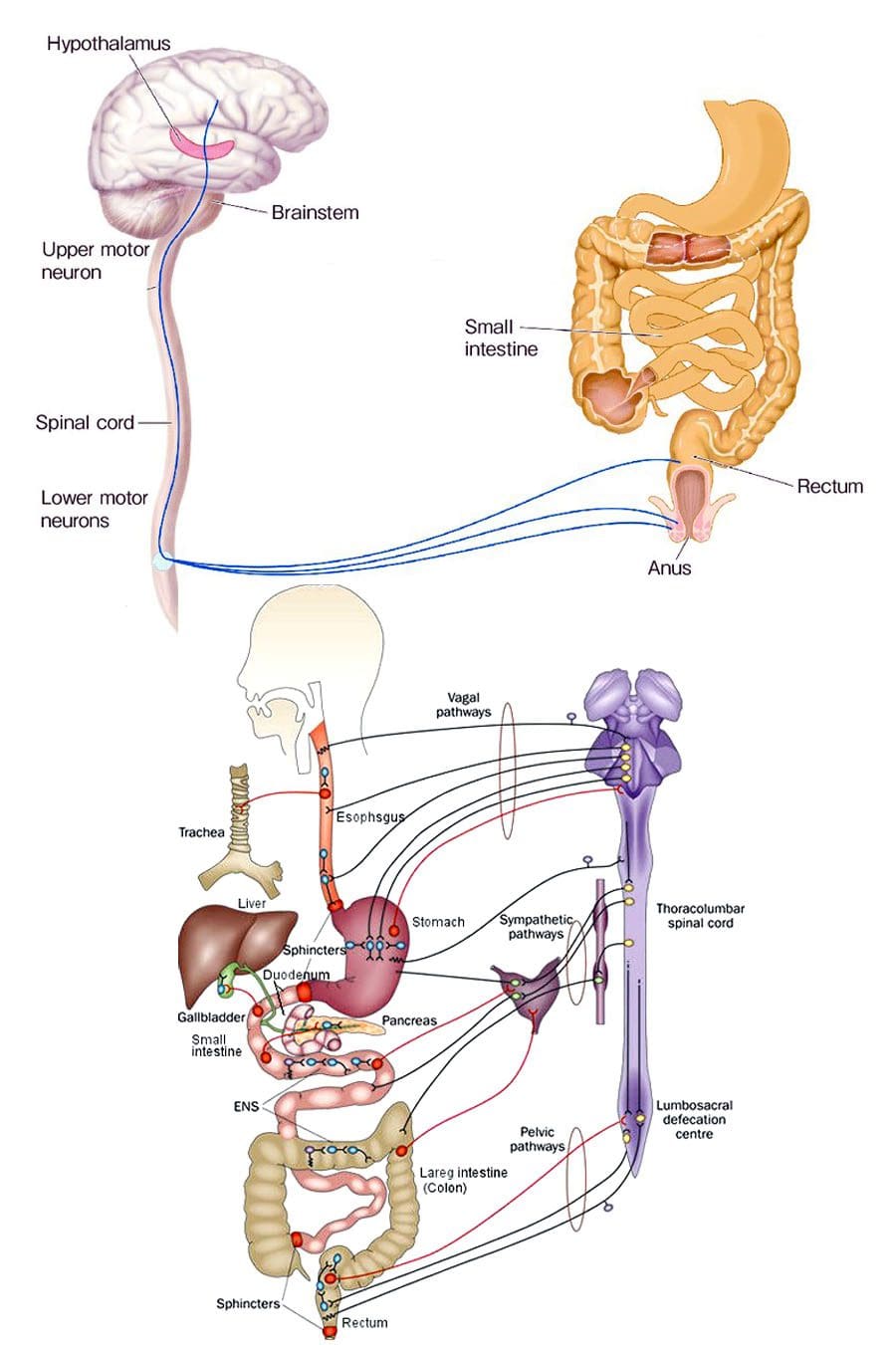
Chiropractic treats the spine that is essential to the function of the central nervous system, which is responsible for digestion. When the nervous system is not functioning correctly, the other systems begin to malfunction. Chiropractic manual and motorized spinal decompression can help with digestion by releasing trapped gas from joints while improving blood circulation that is natural and non-invasive.
Spinal Decompression and Digestion
Spinal alignment and digestion are closely connected. The nerves in the thoracic and lumbar regions affect digestion. When the spine is out of alignment, it stresses the nerves. Nerves that are pinched or constricted are inhibited/disrupted from sending the proper signals to the digestive system. This can lead to new or worsening digestive problems. Spinal conditions that can cause digestive issues:
Herniated discs
Ankylosing spondylosis
Spinal cord injuries
Tumors
Studies have found that digestive issues, including discomfort, heartburn, and bloating, have decreased with regular chiropractic and spinal decompression and decreased constipation and irregular bowel movements. This comes from chiropractic reactivating the body’s natural ability to heal itself.
Increased Circulation
When the spine gets decompressed, it opens up the spine to circulate fluids throughout the body.
This flushes the lymphatic system, increasing the immune system’s function.
Increasing the circulation also provides additional oxygen and nutrients to the brain, improving signaling, memory, and concentration.
Improved Digestion
Poor posture compresses the abdomen and cramps the space the gastrointestinal tract needs to process food properly.
Decompressing the spine and correcting posture allows room for the muscles to contract, expand, and properly circulate waste.
Bowel Program
Treatment focuses on preventing further injuries and helping improve the individual’s quality of life. A doctor, chiropractor, health coach, or nutritionist can recommend a bowel program to help retrain the body to maintain regular bowel movements. These programs are personalized to the individual’s specific condition that takes into account:
Level of the spine injury or condition
Food and drink intake
Bowel movement pattern
Digestive problems
General health
Individual preferences
A bowel program sets up the timing of food intake, fluid intake, medications, and techniques to help bowel movements. The objective is to prevent spontaneous bowel movements, help pass stools regularly, and empty the rectum daily.
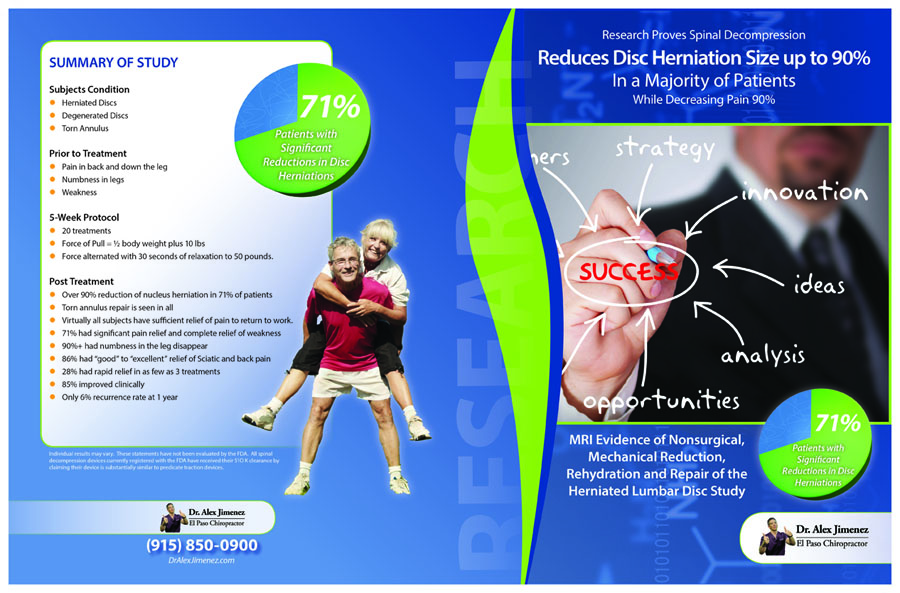
Spinal Decompression Reduced Disc Herniation UP To 90%
DRX9000 Decompression Treatment
References
Browning, Kirsteen N, and R Alberto Travagli. “Central nervous system control of gastrointestinal motility and secretion and modulation of gastrointestinal functions.” Comprehensive Physiology vol. 4,4 (2014): 1339-68. doi:10.1002/cphy.c130055
Holmes, Gregory M, and Emily N Blanke. “Gastrointestinal dysfunction after spinal cord injury.” Experimental neurology vol. 320 (2019): 113009. doi:10.1016/j.expneurol.2019.113009
Kehl, Amy S et al. “Relationship between the gut and the spine: a pilot study of first-degree relatives of patients with ankylosing spondylitis.” RMD open vol. 3,2 e000437. 16 Aug. 2017, doi:10.1136/rmdopen-2017-000437
Lara, Francisco Javier Pérez et al. “Chronic abdominal syndrome due to nervous compression. Study of 100 cases and proposed diagnostic-therapeutic algorithm.” Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract vol. 19,6 (2015): 1059-71. doi:10.1007/s11605-015-2801-8
Neurophysiology: There are two ways that nociceptive information reaches the central nervous system. One is the neospinothalamic tract for quick pain and two is the paleospinothalamic tract for slow pain that increases.
Neurophysiology Of Pain Part II
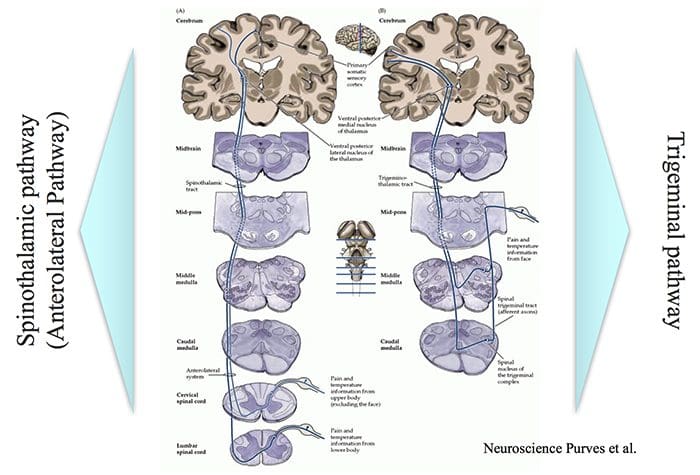
Intensity, Location & Quality of Pain…
… involve Spinothalamic and Trigeminal Pathways
The trigeminal pathway brings information from the face area.
The spinothalamic pathway brings information from the rest of the body.
Both these pathways project to the sensory cortex, which also receives information on innocuous stimuli such as touch, pressure and warmth via a separate pathway.
2 Pain Transmission Pathways For Location Intensity Quality
There is difference between the objective and subjective aspects of injury and pain.
Despite similar injury, people can differ in how much pain they feel.
Depending on the context, pain may not be felt despite injury, e.g. battlefield injury, during intense sports.
This suggests that there is a physiological mechanism that controls the transmission of nociceptive signals to the brain or modifies the interpretation of pain.
The pain control system can also explain the placebo effect.
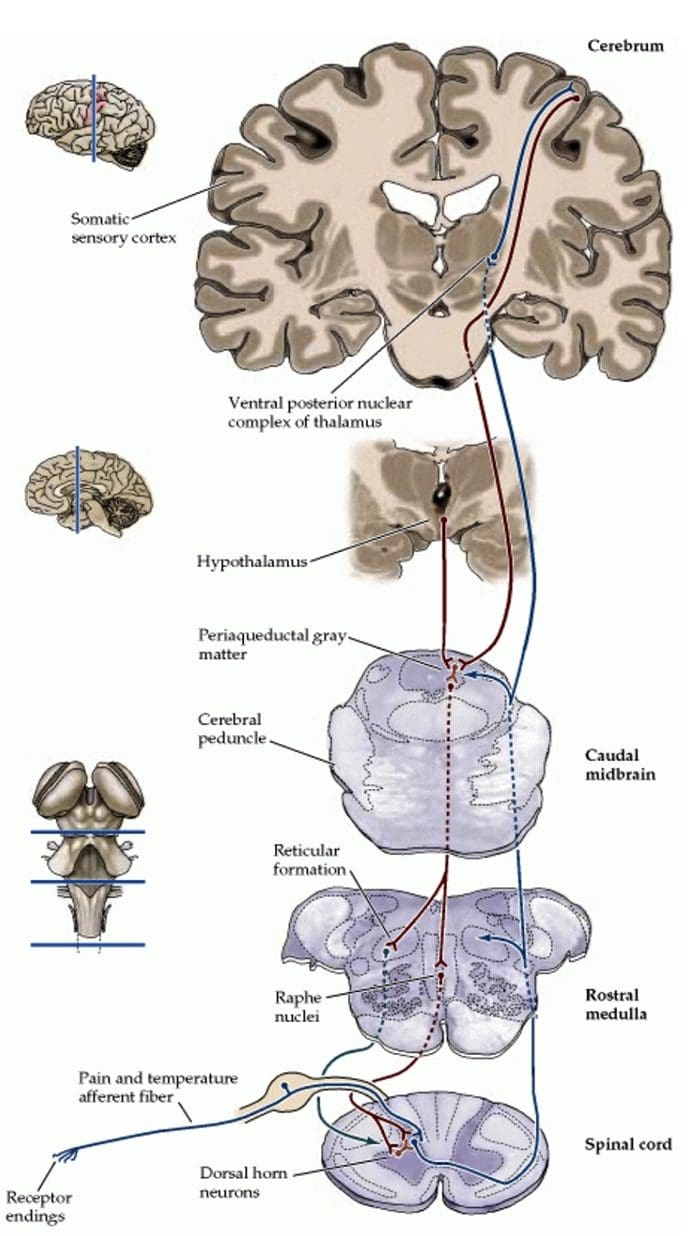
Pain Modulation Pathway
Nerve signals are sent form the somatic sensory cortex and hypothalamus to the periaqueductal gray matter (PAG).
PAG sends signals to the parabrachial nucleus, medullary reticular formation, locus coeruleus, and Raphe neulei.
These in turn can control the in the transmission of nociceptive signals from the spinal cord to the brain.
This involves different involves different neurotransmitters.
Endogenous Opioids
Internally produced molecules with opioid-like action which regulate transmission of nociceptive signals.
Three classes of these molecules have been identified. All are peptide molecules
Enkephalins
Endorphins
Dynorphins
Despite these being powerful, endogenous modifiers of nociceptive signals, it has been difficult to produce and administer them in a way than can used in clinical practice.
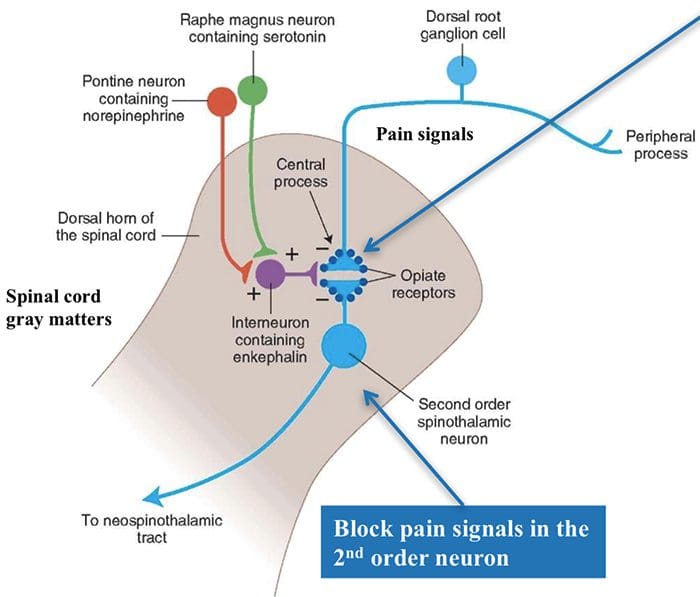
Location Of Nerve Cells With Endogenous Opioid Receptors
In the spinal cord, endogenous opioids can prevent transmission between 1st order nerve cells (bringing signals from the periphery) and 2nd order spinal nerve cells that transmit the signals to the brain.
Also can prevent the increased synaptic efficiency, which plays a role in hyperalgesia.
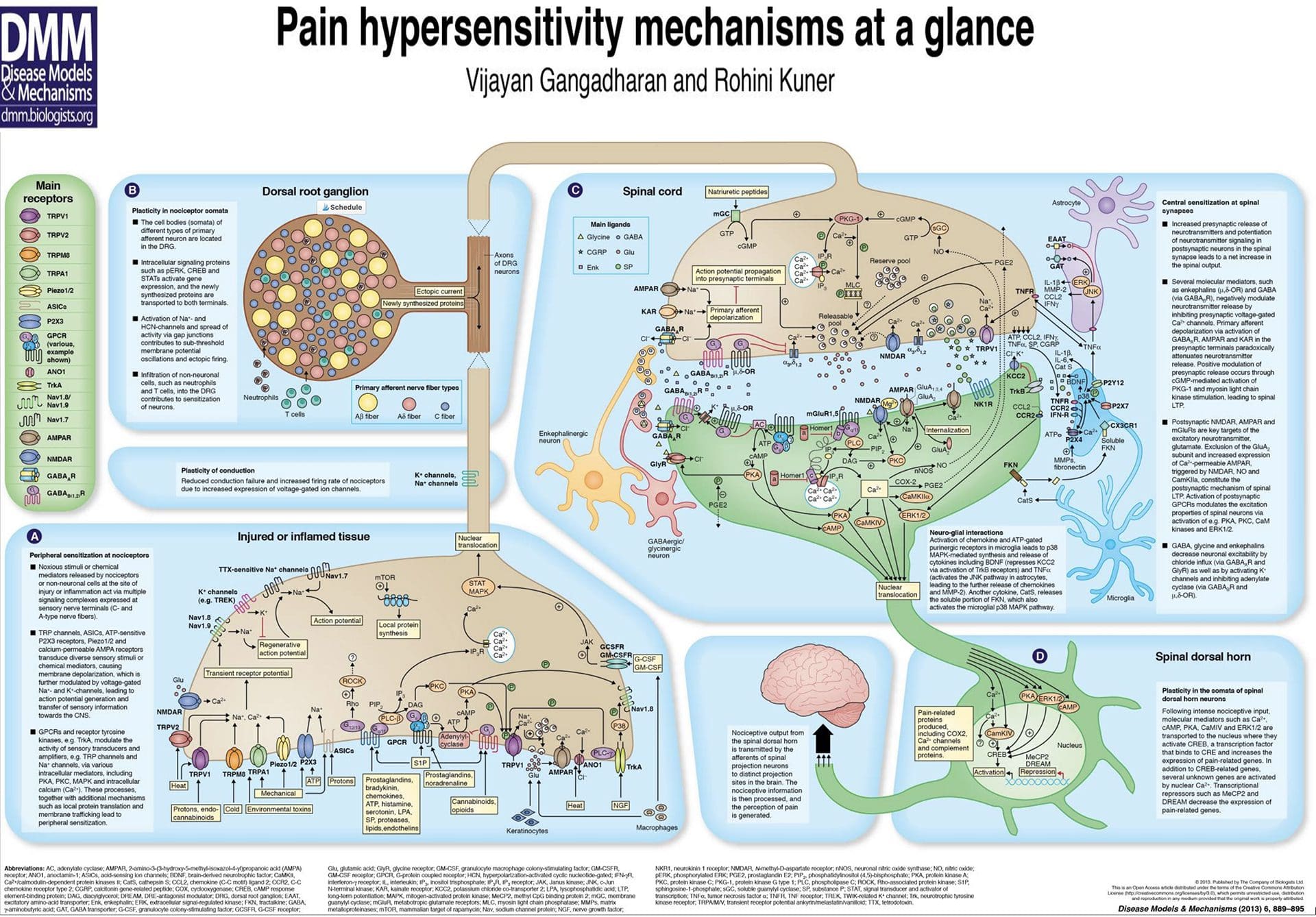
Knowing the molecules involved in the �inflammatory soup� and how they are synthesized provides possible targets for pain reduction.
e.g. prostaglandins are produced by the COX enzyme. The activity of this enzyme is blocked by non-steroidal anti- inflammatory drugs (NSAIDs) such as ibuprofen, diclofenac.
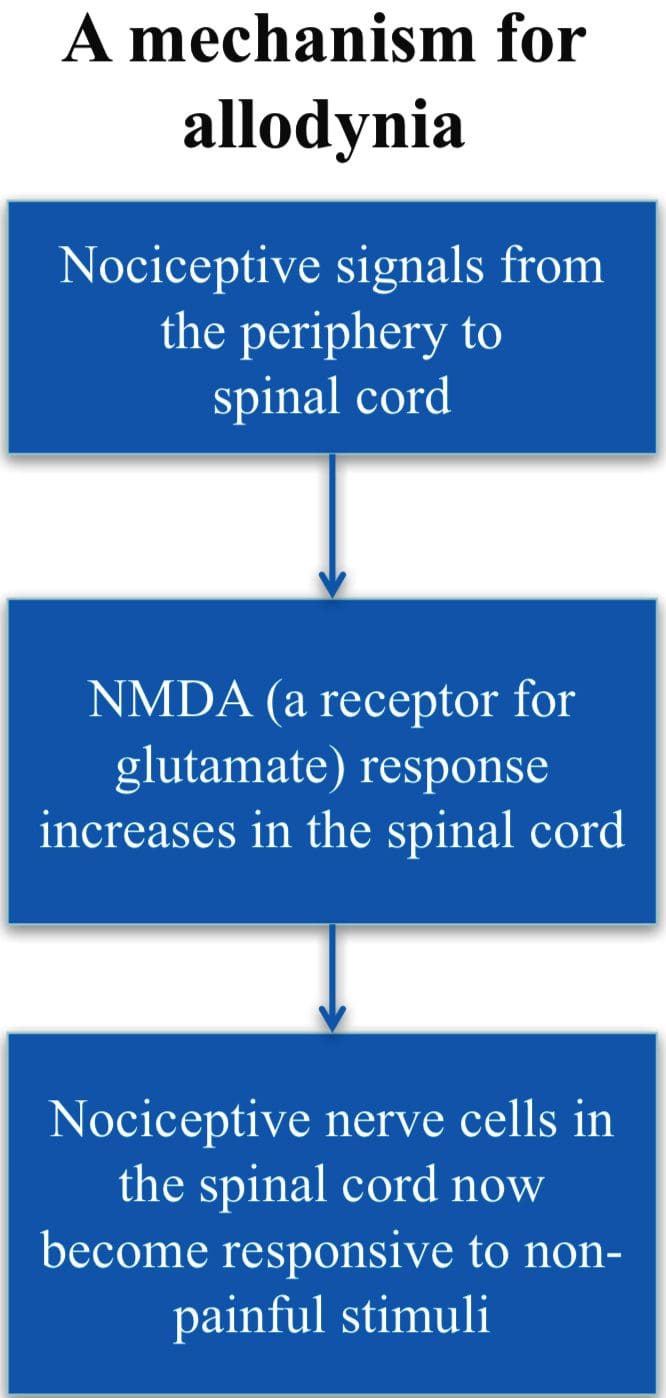
Allodynia
A condition when normally non- painful stimuli cause pain, e.g., touch, light pressure, cold.
Involves changes in the synaptic sensitivity of the nociceptive neurons in the spinal cord (central sensitization).
Drugs such as ketamine, block NMDA receptors and so reduce transmisison of the nociceptive stimuli.
Gate Control Theory of Pain
Mother says to child, �Come I will rub the area which is painful and this will make it feel better.�
After stubbing a toe, we instinctively rub the area; this reduces the sensation of pain.
Ronald Melzack and Patrick Wall in 1962 provided an possible explanation for this effect.
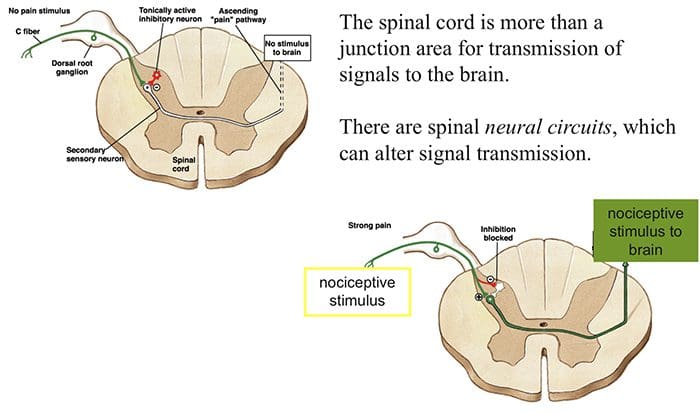
Ascending Tracts | Pain Modulation: Gate Control Theory
Gate Theory
Rubbing the area that hurts stimulates receptors of innocuous stimuli like touch, pressure and vibration.
These mechano-receptors send signals along the A? nerve fibers that:
(1) stimulate spinal nerves (inhibitory inter-neurons) that in turn inhibit signaling in the 2nd order neurons (projection neuron) and (2) directly inhibit the 2nd order neuron to reduce or stop pain signal from being sent to the brain
Transcutaneous Nerve Stimulation (TENS) is based on the Gate Control Theory. Nerves of the innocuous sensory system are stimulated and they in turn, inhibit transmission of nociceptive stimuli in the spinal cord.
Abnormalities Of Pain System
Phantom Pain
Patients with amputation often have burning or tingling pain in the body part removed.
One possible cause is that nerve fibers at the stump are stimulated and the brain interprets the signals as originating in the amputated portion.
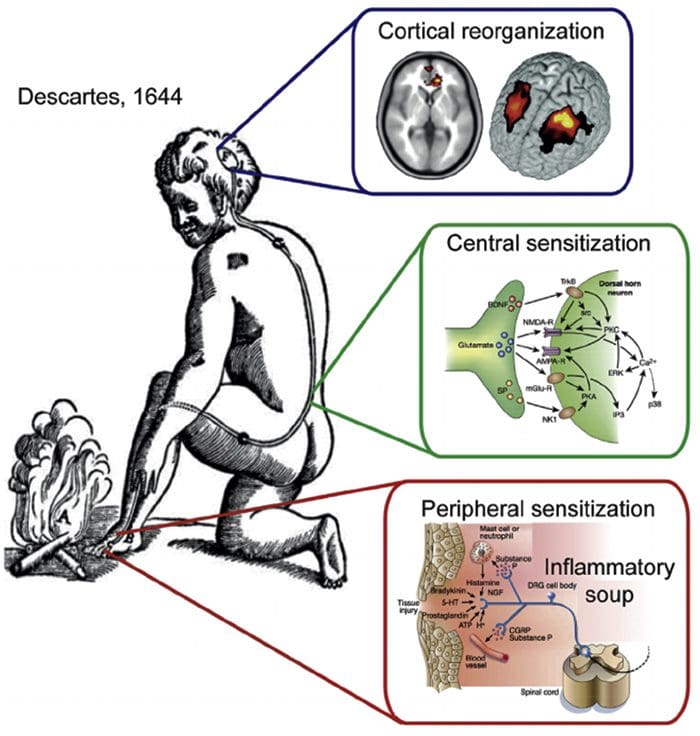
The other is the rearrangement within the cortical areas so that area say for the hand now responds to signals from other parts of the body but still interprets them as coming for the amputated hand.
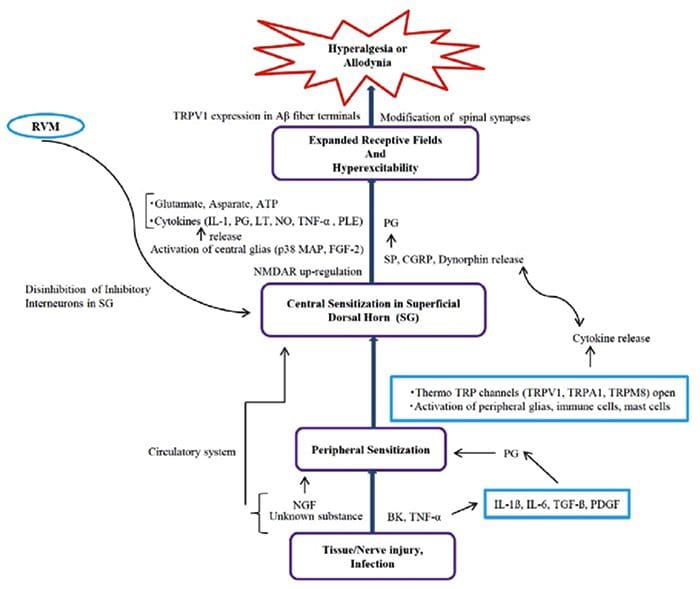
Peripheral Sensitization
Peripheral sensitization represents a reduction in the threshold and/or an increase in magnitude of responsiveness at the peripheral ends of sensory nerve fibers.
This occurs in response to chemical mediators released by nociceptors and non-neuronal cells (e.g. mast cells, basophils, platelets, macrophages, neutrophils, endothelial cells, keratinocytes and fibroblasts) at the site of tissue injury or inflammation.
Basically, it is an increased sensitivity to an afferent nerve stimuli.
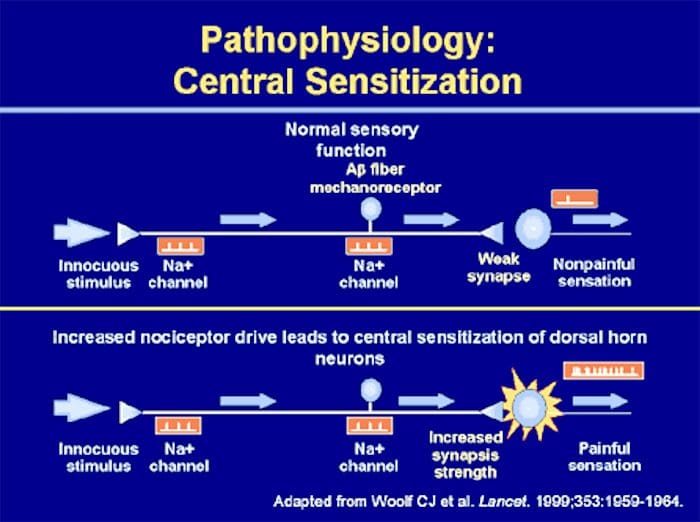
Central Sensitization
Peripheral & Central Sensitisation
A condition of the nervous sytem that is associated with the development and maintenance of chronic pain.
Known as �wind-up� or persistent high reactivity.
�Plastiticity in pain pathways� or the persistence of pain even after an injury has healed.
Is this negative or positive plasticity?
Central Sensitization & C Fibers
Two Main Characteristics Of Central Sensitization:
� Allodynia � occurs when a person experiences pain with things that are normally not painful, ie, soft touch causes pain.
� Hyperalgesia � occurs when a stimulus that is typically painful is perceived as more painful that it should be, ie, a simple bump.
Both are due to hyperreactivity of the nervous system.
Neurophysiology of pain: Pain�defined is the unpleasant sensation that accompanies injury or near injury to tissues, though it can also occur in the absence of such damage if the nociception system is not functioning. Nociception means the system that carries pain signals of injury from the tissues. This is the physiological incident that comes with pain.
Neurophysiology Of Pain
Objectives
Basics of the nervous system
Synaptic function
Nerve impulses
Transduction of peripheral painful stimuli
Central pathways
Central Sensitization
PeripheralSensitization
Control or modulation of pain signals
Pathophysiology of pain signaling pathway
Definition Of Pain
“Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”.
It is important to know the basic structure of the nervous system.
This will help in:
� Understanding the mechanism by which nociceptive signals are produced.
� Know the different regions of the nervous system involved in processing these signals.
� Learn how the different medications and treatment for pain management work.
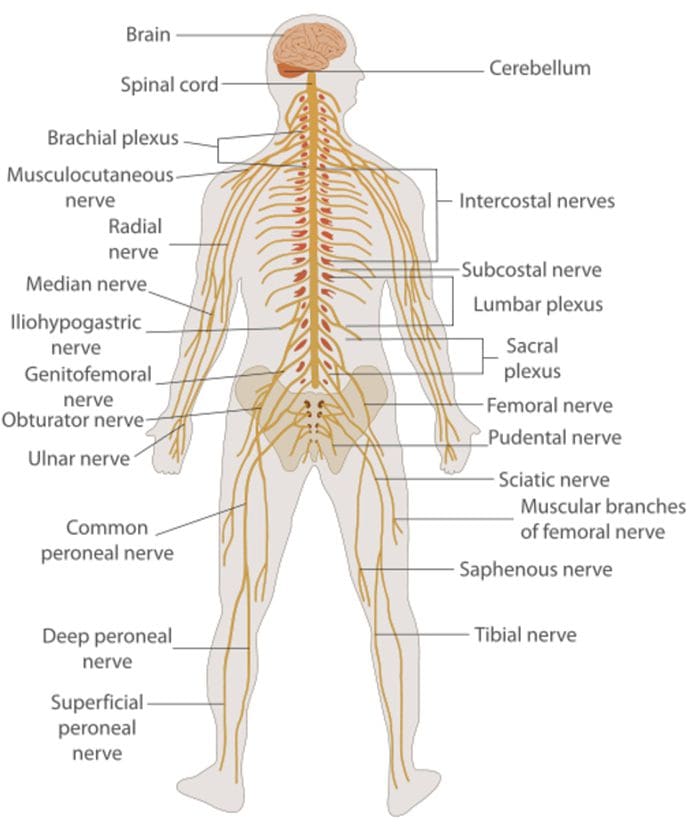
Nervous System
Central nervous system (CNS)
Brain and Spinal Cord
Peripheral Nervous System (PNS)
Nerve fibers go to all parts of the body.
Send signals to the different tissues and send signals back to the CNS.
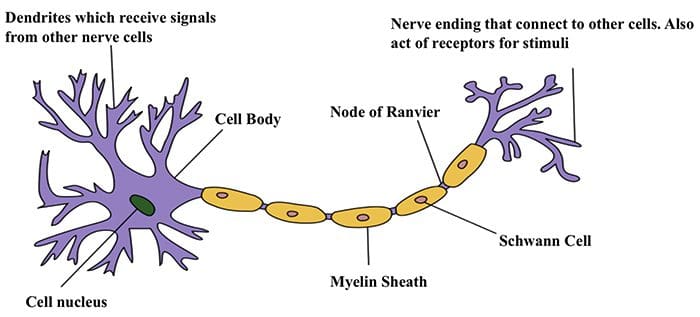
Nerve Cells
The nervous system is made up of nerve cells which send long processes (axons) to make contact with other cells.
Nerve Cell-To-Nerve Cell Communication
Nerve cells communicate with other cells by releasing a chemical from the nerve endings � Neurotransmitters
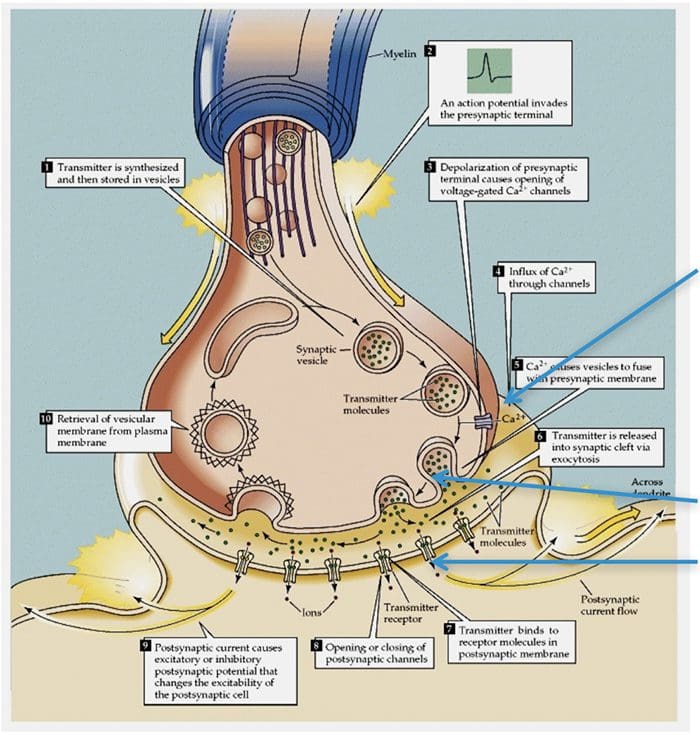
Basic Steps In Synaptic Transmission
Synaptic Transmission
Steps in the passage of signal from one nerve cell to other.
Drugs are used to block the transmission of signals from one nerve cell to other.
These drugs can effect:
Ca2+ ion channel to prevent Ca2+ inflow which is essential for neurotransmitter (NT) release, e.g., the action of gabapentin.
Release of NT.
Prevent NT from binding to its receptor so stop further transmission of the signal.
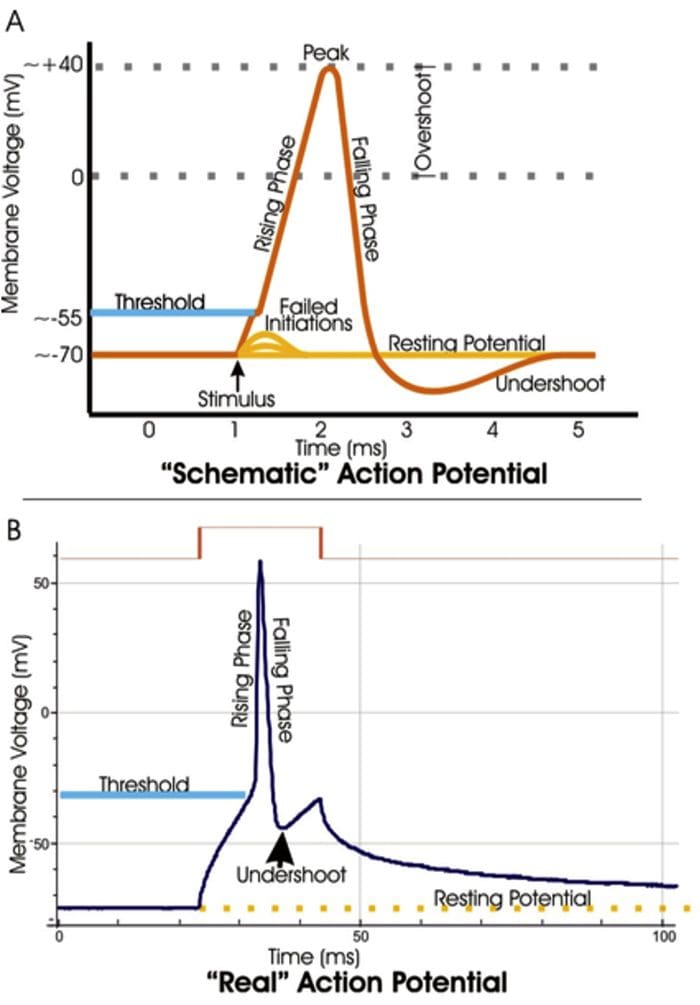
Electrical Impulse
Signals move along a nerve process (axon) as a wave of membrane depolarization called the Action Potential.
The inside of all nerve cells has a negative electrical potential of around � 60 mV.
When stimulated this negative electrical potential becomes positive and then negative again in milliseconds.
The action potential moves along the nerve process (axon) to the nerve ending where it cause release of NT.
Action Potential
When there is no stimulation the membrane potential is at its Resting Potential.
When stimulated, channels in the nerve membrane open allowing the flow of sodium ions (Na+) or calcium ions (Ca2+) into the nerve or cell. This makes the inside less negative and in fact positive -the peak of the action potential (+40 mV).
These channels than close and by the opening of K+ channels the membrane potential returns to its resting level.
Stopping Action Potentials To Stop Nociceptive Stimuli
Nociceptive stimuli are those that will create a sensation of pain after they are processed in the CNS.
Nociceptive signals can be prevented from reaching the CNS by blocking the action of the channels that control the movement of ions across the nerve membrane.
A number of anesthetic agents stop Na+ channel from working and hence stop the generation of actions potentials and transmission of signals to the CNS.
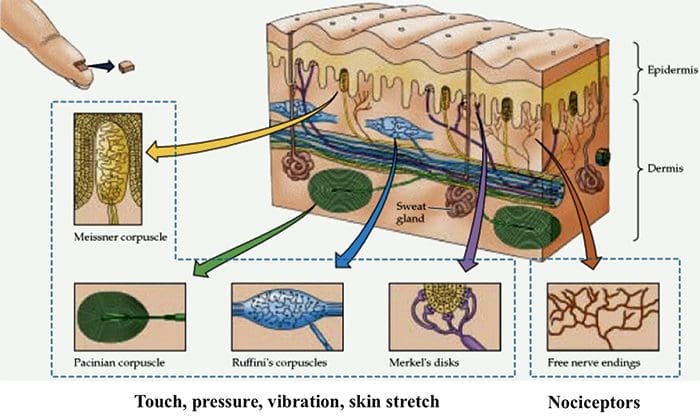
Sensory Systems
The sensory system that can be divided into two divisions:
A Sensory System that transmits innocuous stimuli such as touch, pressure, warmth.
A System that transmits stimuli that indicate that tissues have been damaged = nociceptive .
These two systems have different receptors and pathways in the PNS & CNS
Nociceptors are free nerve endings that respond to stimuli that can cause tissue damage or when tissue damage has taken place.
Present in membrane of free nerve endings are receptors (protein molecules) whose activity changes in the presence of painful stimuli.
(Note the use of the same term receptor is used for cell or organs or molecules that involved in transduction of a stimuli.)
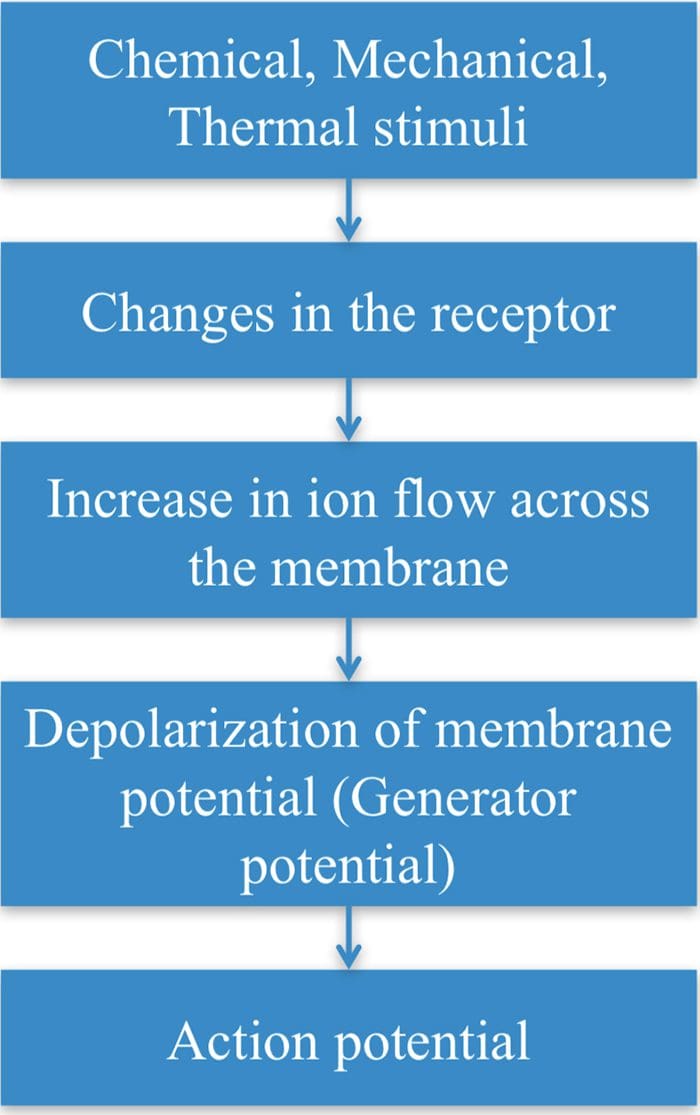
Transduction
Transduction is the process of converting the stimuli into a nerve impulse.
For this to occur the flow of ions across the nerve membrane has to change to allow entry of either Na+ or Ca2+ ions to cause depolarization of the membrane potential.
This involves a receptor molecule that either directly or indirectly opens the ion channels.
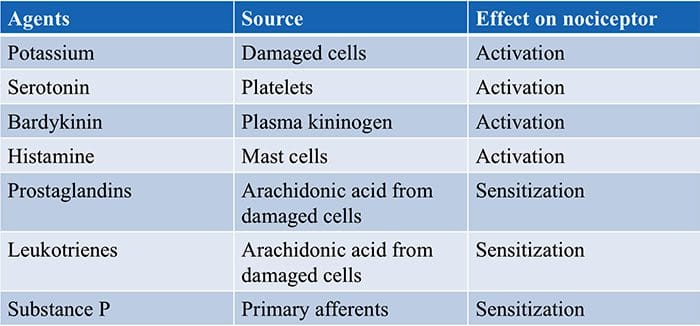
Chemical Agents…
… which can cause the membrane potential at the free nerve ending (nociceptor) to produce an action potential.
Many stimuli � mechanical, chemical and thermal � give rise to painful sensation making transduction a complex process.
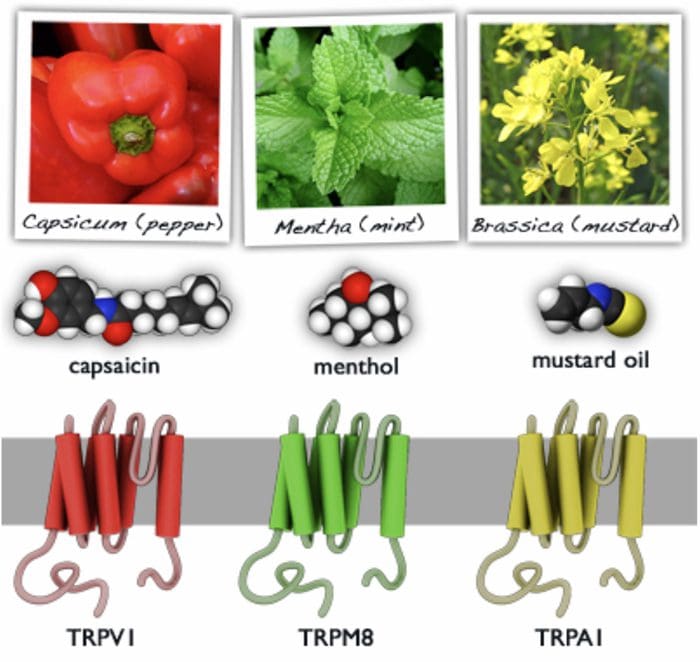
Recently receptor molecules have been identified�� Transient Receptor Potential (TRP) channels � that respond to a number of strong stimuli.
TRP receptors are also involved in transmitting the burning sensation of chili pepper.
In time, drugs that act on these receptors will be developed to control pain.
Different TRP Channels
Capsasin, the active ingredient in chili pepper, is used in patches for relief of pain.
Menthol and peppermint gels are used to relieve muscle pain.
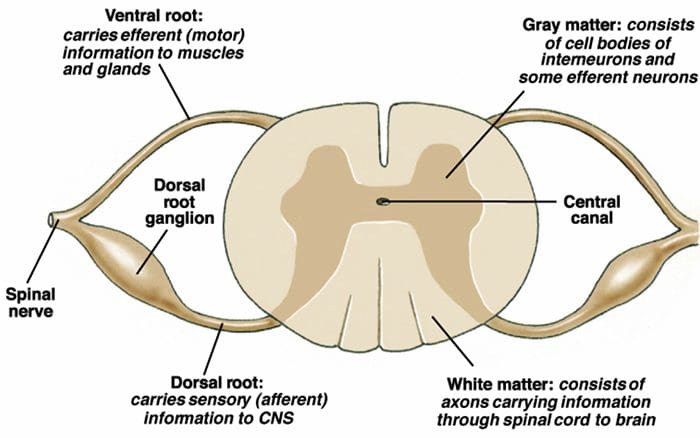
Motor Output & Sensory Input To Spinal Cord
Sensory nerves have their cell body outside the spinal cord in the dorsal root ganglia ( = 1st order neurons).
One process goes to the periphery, the other goes to the spinal cord where it makes synaptic contact with nerve cells in the spinal cord ( = 2nd order neurons).
The 2nd order neuron sends processes to other nerve cells in the spinal cord and to the brain.
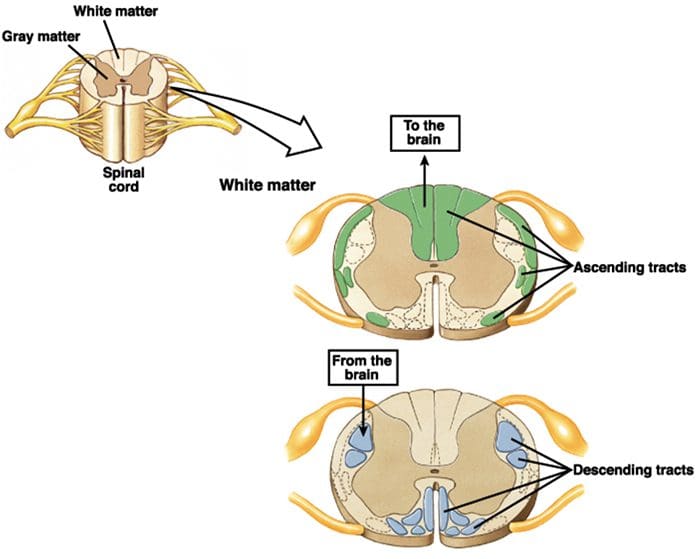
2nd Order Nerve Cells Send Nerve Fibers In The Spinal Cord White Matter
Transmission Of Nociceptive Signals From The Periphery To The Brain
Silverthorn
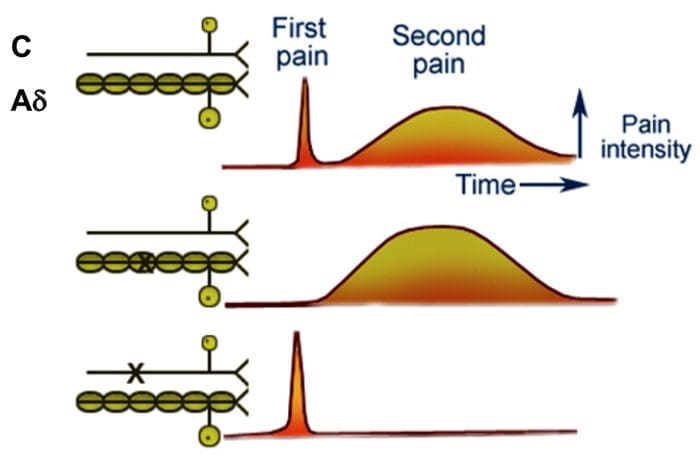
A Delta (?) & C Nerve Fibers
Nerve fibers are classified according to the:
� (1) diameter of the nerve fiber and
� (2) whether myelinated or not.
A? and C nerve fiber endings respond to strong stimuli.
A? are myelinated and C are not.
Action potentials are transmitted 10 times faster in the A?
(20 m/sec) fibers than in C fibers (2 m/sec).
A? & C fibers
A? fibers respond mainly to mechanical and mechno-thermal stimuli.
C fibers are polymodal, i.e. the nerve ending responds to several modalities � thermal, mechanical and chemical
This polymodal ability is due to the presence of different receptor molecules in a single nerve ending.
Fast & Slow Pain
Most people when they are hit by an object or scrape their skin, feel a sharp first pain (epicritic) followed by a second dull, aching, longer lasting pain (protopathic).
The first fast pain is transmitted by the myelinated A? fibers and the second pain by the unmyelinated C fibers.
Central Pain Pathways
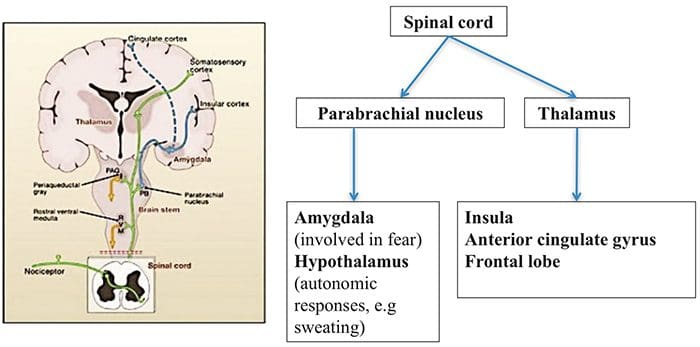
Nociceptive signals are sent to the spinal cord and then to different parts of the brain where sensation of pain is processed.
There are a pathways/regions for assessing the:
Location, intensity, and quality of the noxious stimuli
Unpleasantness and autonomic activation (fight-or-flight response, depression, anxiety).
Dr. Sletten Discussing Central Sensitization Syndrome (CSS)
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Brain Areas Involved In Processing Of Nociceptive Signals
Brain Areas Involved In Processing Of Nociceptive Signals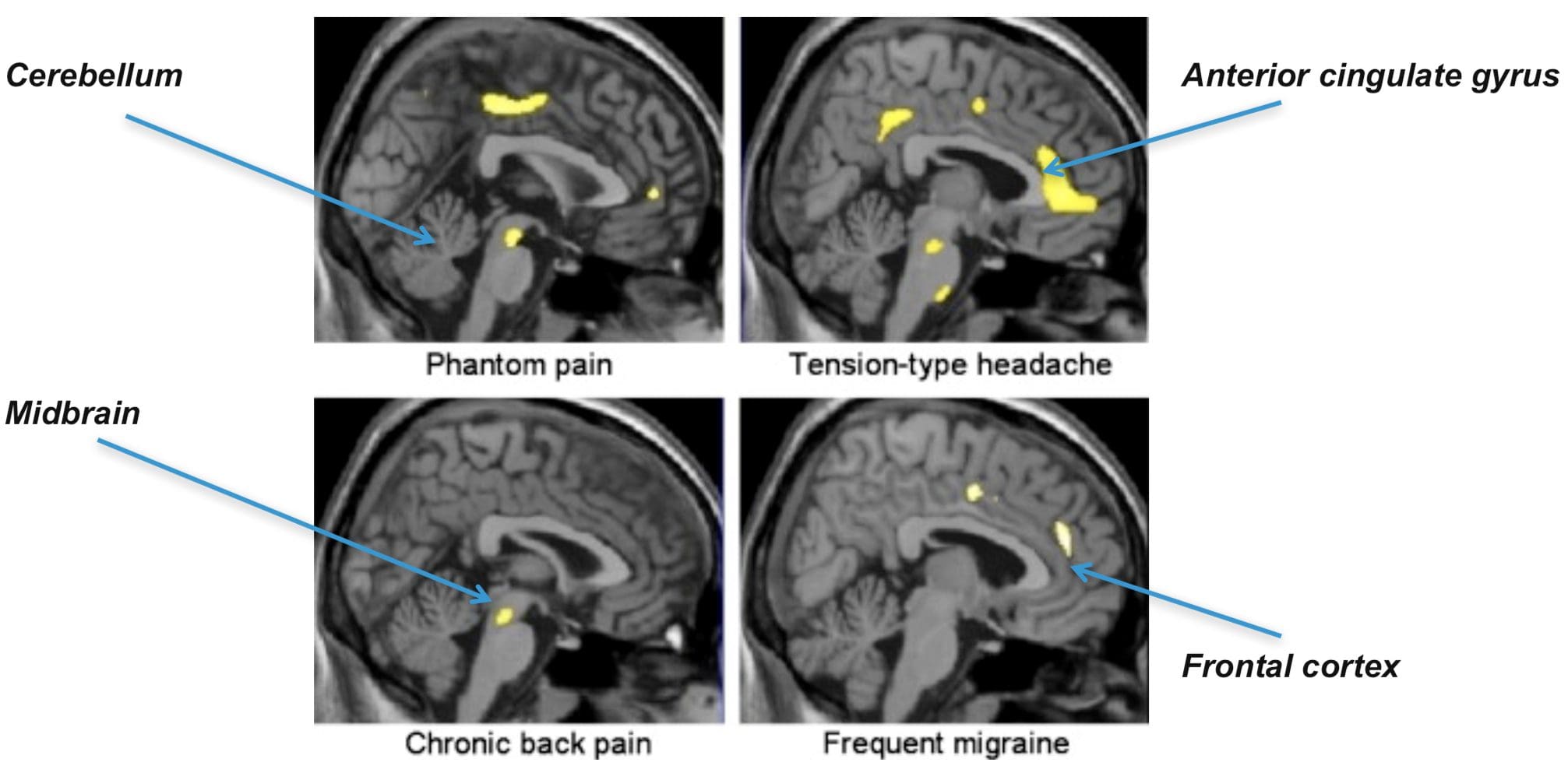 The Anterior Cingulate & Insula Cortex Are Activated In Human Subjects
The Anterior Cingulate & Insula Cortex Are Activated In Human Subjects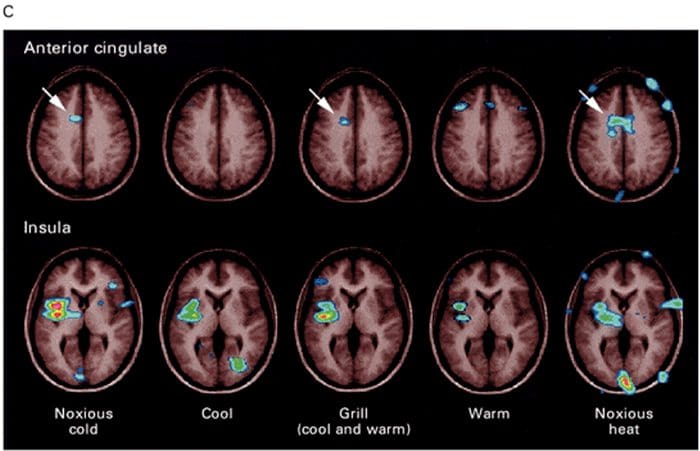
 Inflammatory Soup – Hyperalgesia
Inflammatory Soup – Hyperalgesia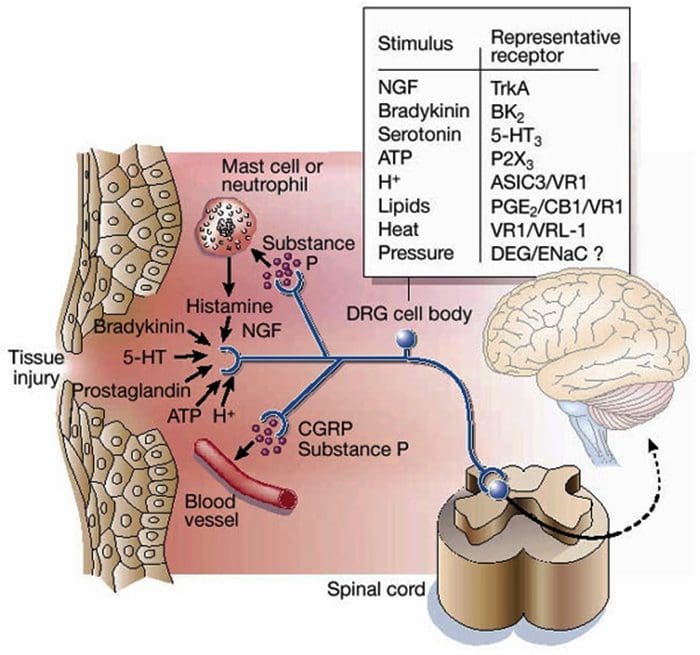
 Gate Control Theory of Pain
Gate Control Theory of Pain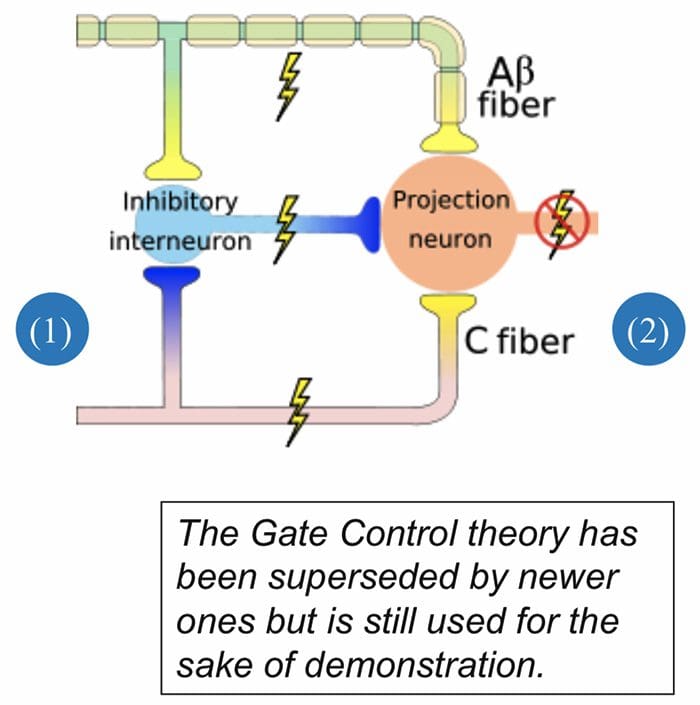
 Abnormalities Of Pain System
Abnormalities Of Pain System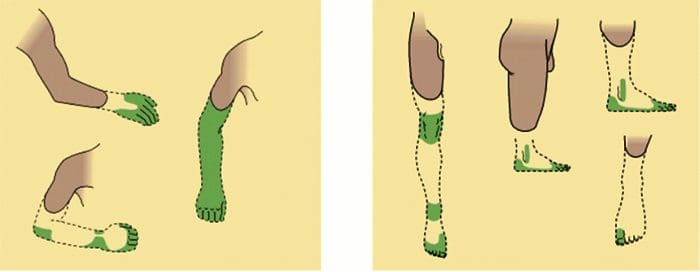 Peripheral Sensitization
Peripheral Sensitization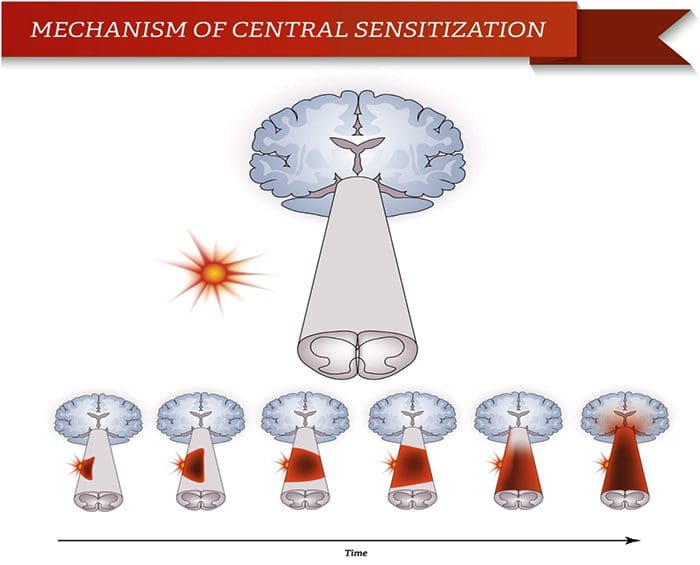
 Somatosensory Cortex Organization
Somatosensory Cortex Organization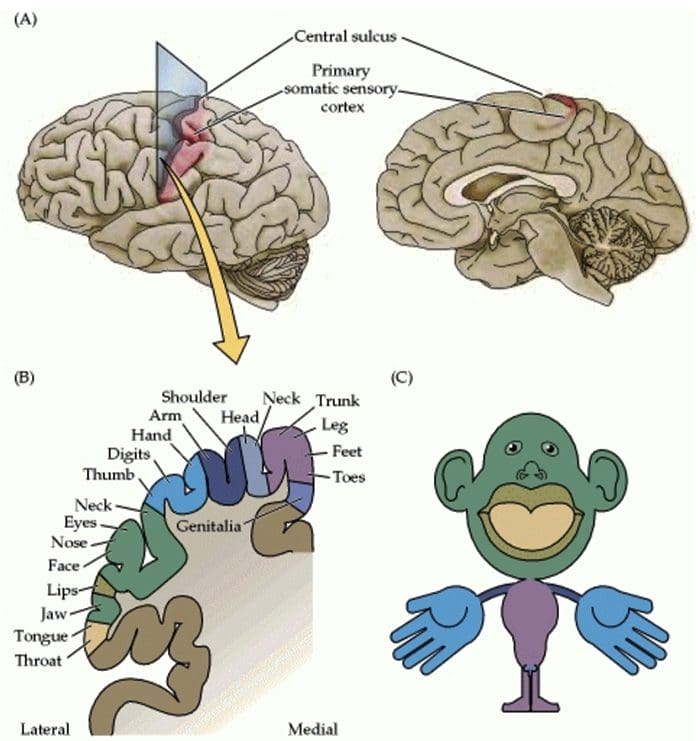 Cortical Reorganization
Cortical Reorganization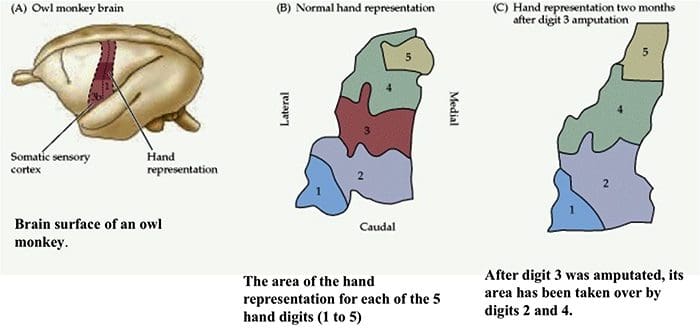
 Nerve Cell-To-Nerve Cell Communication
Nerve Cell-To-Nerve Cell Communication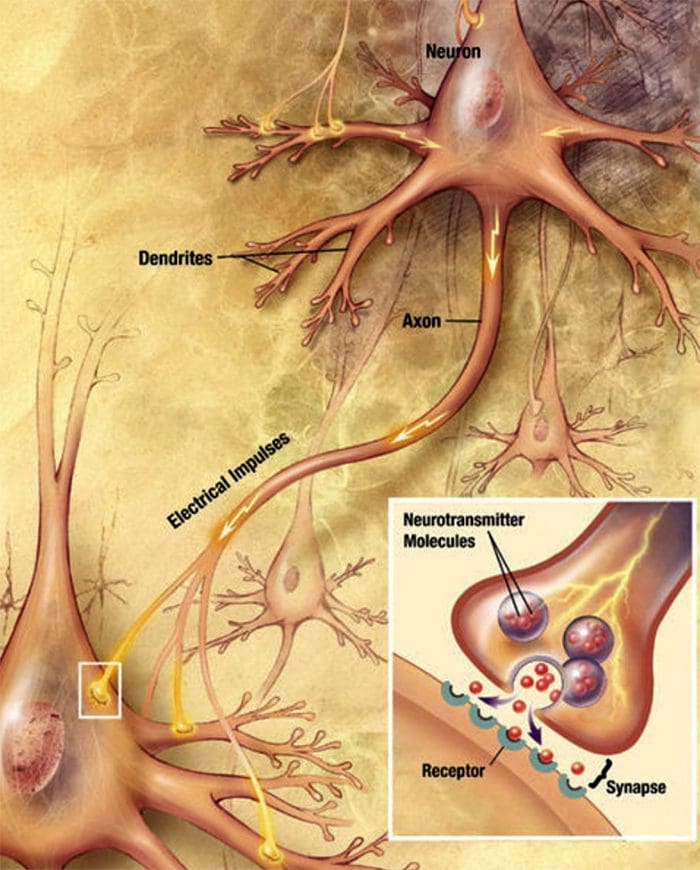 Nerve cells communicate with other cells by releasing a chemical from the nerve endings � Neurotransmitters
Nerve cells communicate with other cells by releasing a chemical from the nerve endings � Neurotransmitters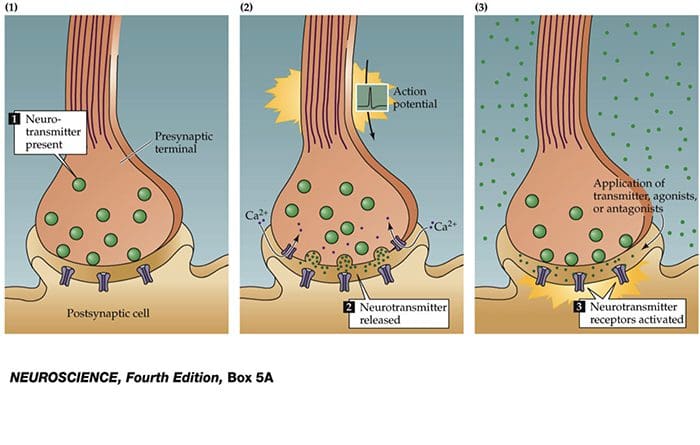
 TRP Channels
TRP Channels