SKULL FX: COMMON IN THE SETTINGS OF HEAD INJURIES. SKULL FX OFTEN POINT TO OTHER COMPLICATING FACTORS: INTRA-CRANIALHEMORRHAGING, CLOSED TRAUMATIC BRAIN INJURY AND OTHER SERIOUS COMPLICATIONS
SKULL X-RAYS ARE VIRTUALLY OBSOLETE IN EVALUATING HEAD INJURY. CT SCANNING W/O CONTRAST IS THE MOST IMPORTANT INITIAL STEP IN EVALUATION OF ACUTE HEAD TRAUMA. MRI HASA POOR ABILITY TO REVEAL SKULL FRACTURES, AND NOT TYPICALLY USED FOR AN INITIAL DX OF ACUTE HEAD TRAUMA.
SKULL FX ARE IDENTIFIED AS FXS OF SKULL VAULT, SKULL BASE AND FACIAL SKELETON EACH ASSOCIATED WITH SPECIFIC FEATURES AND HELP TO PREDICT COMPLICATIONS.
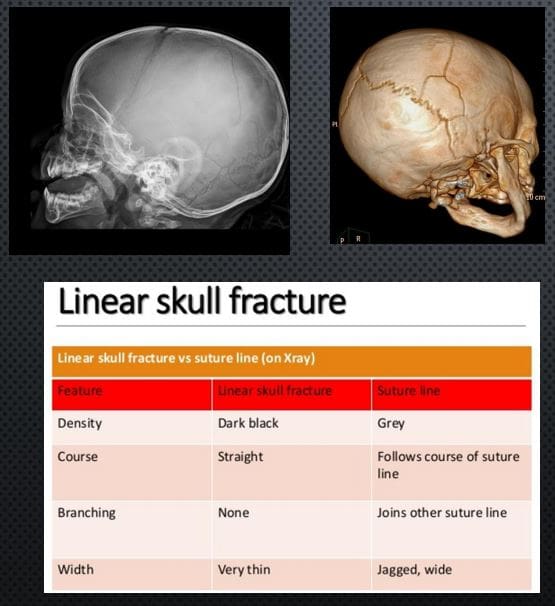
LINEAR SKULL FX: SKULL VAULT. M/C FX. CT SCANNING IS THE KEY TO EVALUATE ARTERIALEXTRADURAL HEMORRHAGING
X-RAY DDX: SUTURES VS. LINEAR SKULL FX. FX IS THINNER, �BLACKER� I.E. MORE LUCENT, CROSSESSUTURES,�AND VASCULAR GROOVES, LACKSSERRATIONS
RX: IF NO INTRACRANIAL BLEEDS THAT NO TREATMENT. NEUROSURGICAL CARE IF BLEEDSDETECTED BY CT SCANNING
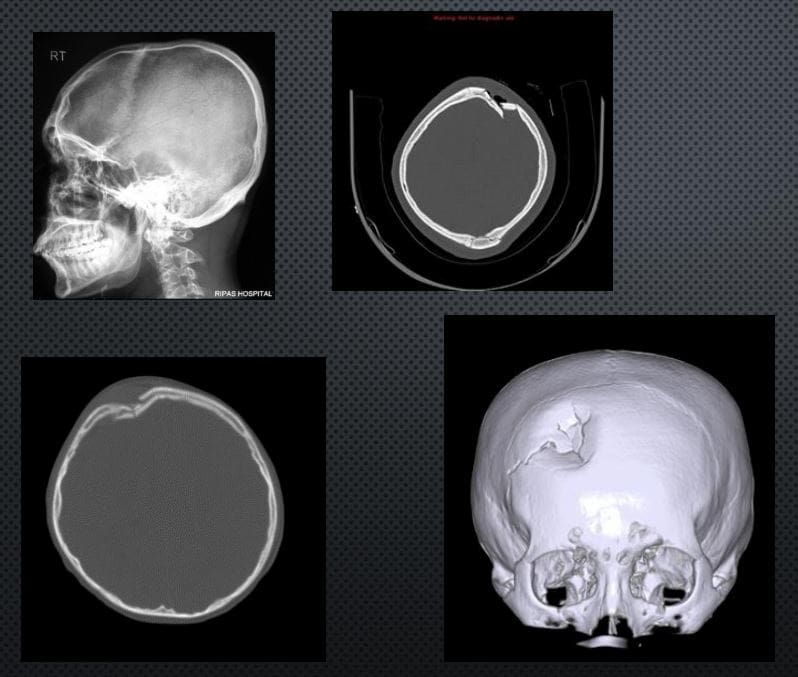
DEPRESSED SKULL FX: 75% IN THE VAULT. CAN BE DEADLY. CONSIDERED AN OPEN FX. MOST CASES NEED NEUROSURGICALEXPLORATION ESPECIALLY IFFRAGMENTS DEPRESSED >1-CM.COMPLICATIONS: VASCULAR INJURY/HEMATOMAS, PNEUMOCEPHALUS, MENINGITIS, TBI, CSF LEAK, BRAIN HERNIATION ETC.
IMAGING: CT SCANNING W/O CONTRAST
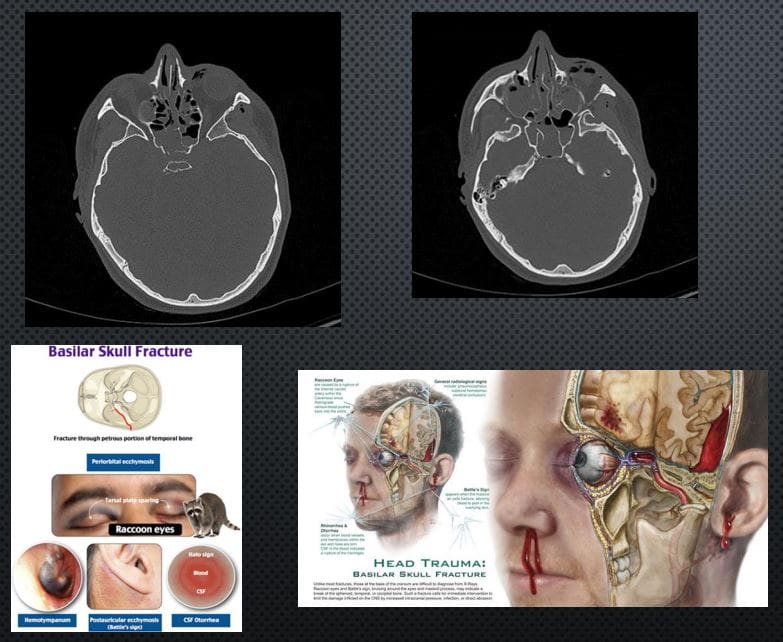
BASILAR SKULL FX: CAN BE DEADLY. OFTEN ALONG OTHER MAJOR HEAD TRAUMA OF THE VAULT AND FACIALSKELETON, OFTEN WITH TBI AND MAJORINTRACRANIAL HEMORRHAGING. OFTEN OCCUR AS �HEADBAND� EFFECT OF IMPACT AND MECHANICAL TENSION THROUGH THE OCCIPUT AND TEMPORAL BONES THROUGH SPHENOID AND OTHER BASE OF SKULL BONES. CLINICALLY: RACCOON EYES, BATTEL SIGN, CSFRHINO/OTORRHEA.
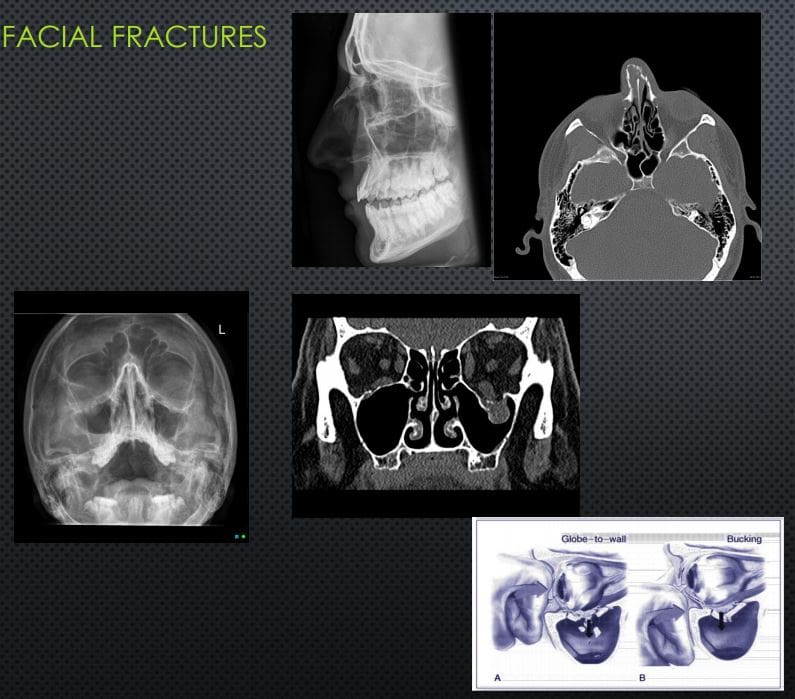
Facial Fractures
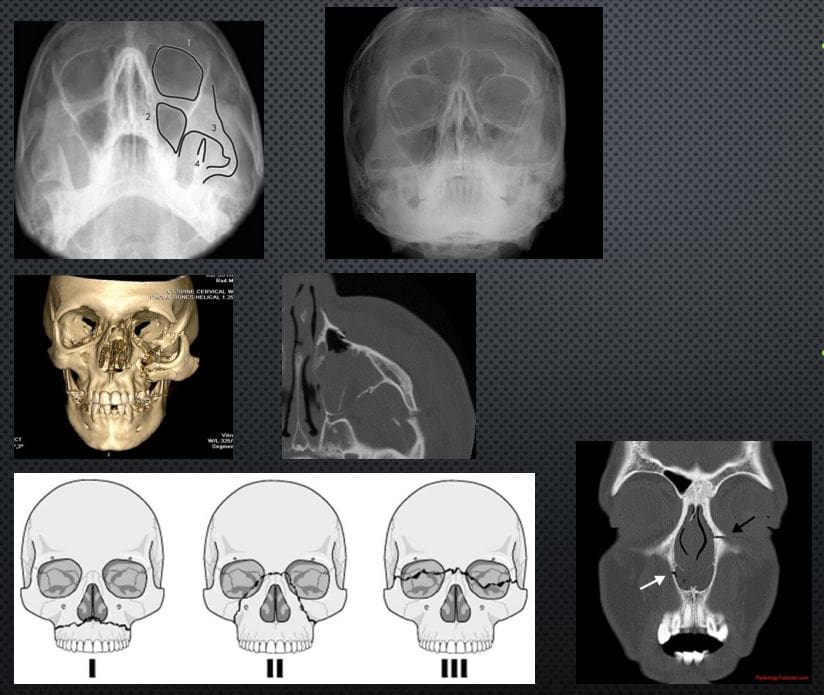
NASAL BONES FX: 45% OF ALLFACEFXM/C IMPACT IS LATERAL(FIST BLOW ETC.) IF UNDISPLACEDNO TREATMENT, IF DISPLACED MAY COMPLICATE AIR FLOW AND RESPIRATORY PASSAGE, MAY BE ASSOCIATED WITH OTHER FACIAL/SKULL INJURY. X-RAYS 80%SENSITIVE, FOLLOWED BY CT INCOMPLEX INJURIES.
ORBITAL BLOW OUT FX: COMMONORBITAL INJURY D/T IMPACT ON THE GLOBE AND/OR ORBITAL BONE. FX OF ORBITAL FLOOR INTOMAXILLARY SINUS VS. MEDIAL WALL INTO ETHMOID SINUS. COMPLICATIONS: ENTRAPPEDINFERIOR RECTUS M, PROLAPSEORBITAL FAT,�AND SOFT TISSUES, HEMORRHAGING AND OPTIC NERVE DAMAGE. RX: CONCERNS OF GLOBE INJURY ARE IMPORTANT, GENERALLY TREATEDCONSERVATIVELY IF NO COMPLICATIONS PRESENT
TRIPOD FX: 2ND M/C FACIAL FX#AFTER NASAL (40% OF MIDFACEFX) 3-POINT FX-ZYGOMATICARCH, ORBITAL PROCESS OF ZYGOMATIC BONE & SIDE OF MAXILLARY SINUS WALL, MAXILLARY PROCESS OF ZYGOMATIC BONE.COMPLICATED BY NERVE INJURY, TEMPORALIS M DAMAGE ETC. CT SCANNING IS MORE INFORMATIVE THAT X-RAYS (WATER�S VIEW).
LEFORT FX: SERIOUS FX ALWAYS INVOLVES PTERYGOID PLATES, POTENTIALLY SEPARATINGMIDFACE AND ALVEOLAR PROCESS WITH TEETH FROM THE SKULL. CONCERNS: AIRWAYS, HEMOSTASIS, NERVE INJURIES. CT SCANNING IS REQUIRED. POTENTIAL RISK OF BASILAR SKULL FX
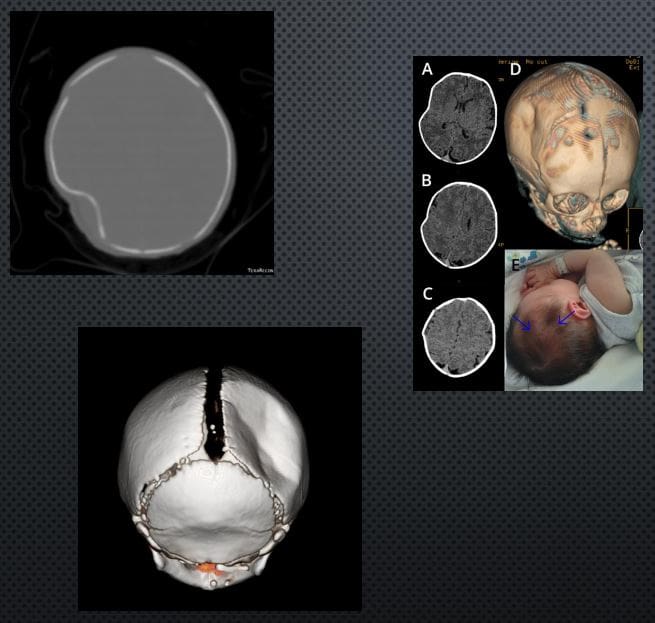
PING-PONG FX:�EXCLUSIVELY IN INFANTS. AN INCOMPLETE FX D/T FOCALDEPRESSION: FORCEPS DELIVERY, DIFFICULT LABOUR ETC. FOCALTRABECULAR MICROFRACTURIINGLEAVING DEPRESSION RESEMBLING APING-PONG. DX IS MAINLY CLINICALSEEN AS FOCAL DEFECT �DEPRESSION� IN THE SKULL. TYPICALLYNEUROLOGICALLY INTACT. CT MAY HELP IF BRAIN INJURY IS SUSPECTED. RX: OBSERVATIONAL VS. SURGICAL IN COMPLICATED INJURIES. SPONTANEOUSREMODELING HAS BEEN REPORTED
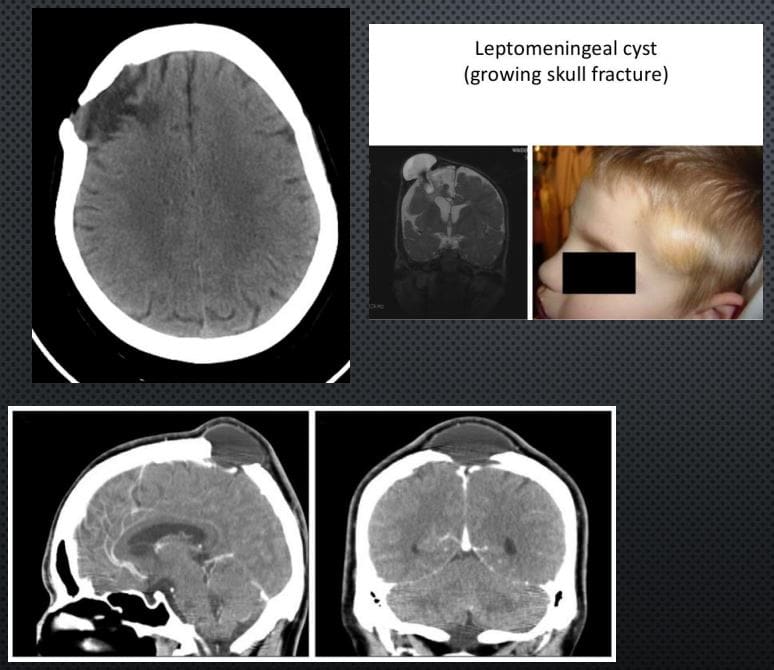
LEPTOMENINGEAL CYST (GROWING SKULL FX)- ARE AN ENLARGING SKULL FRACTURE THAT DEVELOPS ADJACENT TO POSTTRAUMATIC ENCEPHALOMALACIA
IT IS NOT A CYST, BUT AN EXTENSION OF THEENCEPHALOMALACIA THAT SEEN A FEW MONTHS POST-TRAUMA WITH PREVIOUS SKULL FX FOLLOWEDBY HERNIATION OF THE MENINGES AND ADJACENTBRAIN WITH PULSATIONS OF THE CSF. CT IS BEST ATDX THIS PATHOLOGY. INDICATES: GROWING FX AND ADJACENT ENCEPHALOMALACIA AS FOCALHYPOATTENUATING LESION.
DDX: INFILTRATING CELLS/METS/OTHER NEOPLASMSINTO SUTURES, EG, INFECTION ETC.
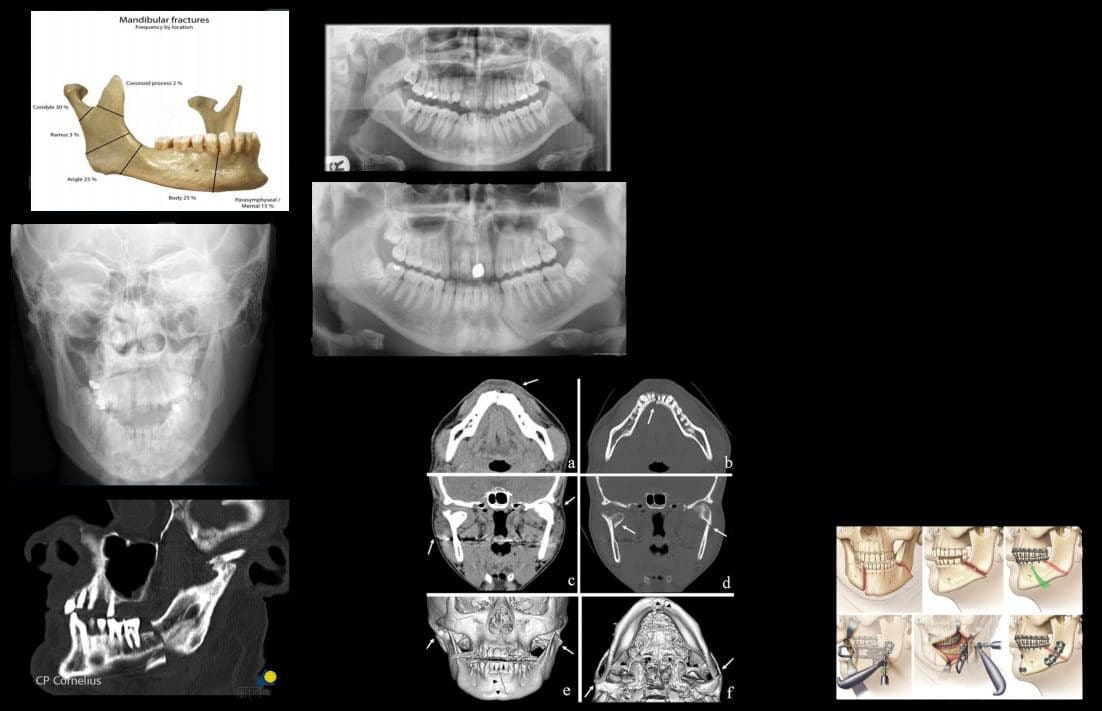
MANDIBULAR FXS: COMMON. POTENTIALLYCONSIDERED AN OPEN FX D/T INTRA-ORALEXTENSION. 40% FOCAL BREAK DESPITEMANDIBLE BEING A RING. DIRECT IMPACT(ASSAULT) M/C MECHANISM
PATHOLOGICAL FX D/T BONE NEOPLASMS, INFECTION ETC. IATROGENIC DURING ORAL SURGERY (TOOTH EXTRACTION)
IMAGING: MANDIBLE X-RAYS, PANOREX, CT SCANNING ESP. IN CASES OF ASSOCIATEDFACE/HEAD TRAUMA
COMPLICATIONS: AIRWAY OBSTRUCTION, HEMOSTASIS IS A MAJOR CONSIDERATION, DAMAGE TO MANDIBULAR N, OSTEOMYELITIS/CELLULITIS AND POTENTIAL SPREAD THROUGH FLOOR OF THE MOUTH (LUDWIGANGINA) AND NECK FASCIAL SOFT TISSUES INTOMEDIASTINUM. CANNOT BE NEGLECTED D/T HIGH MORTALITY RATES.
RX: CONSERVATIVE VS. OPERATIVE
Acute Intracranial Hemorrhage
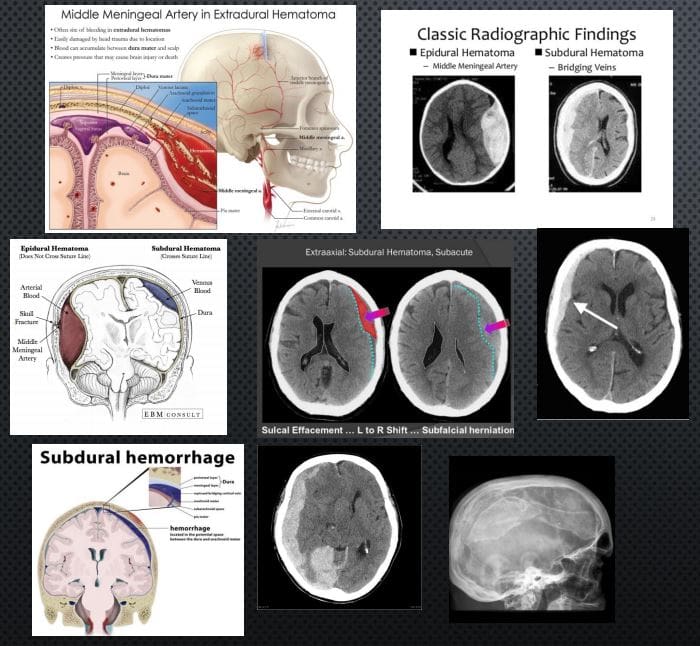
EPI AKA EXTRADURAL: (EDH) TRAUMATIC RAPTURE OF MENINGEAL ARTERIES (MMA CLASSIC) WITH RAPIDLY FORMING HEMATOMA BETWEEN THE INNER SKULL AND OUTER DURA. CT SCANNING IS THE KEY TO DX: PRESENTS AS �LENTIFORM� I.E. BICONVEX COLLECTION OF ACUTE (HYPERDENSE) BLOOD THAT DOES NOT CROSSSUTURES AND HELPS WITH DDX OF A SUBDURAL HEMATOMA. CLINICALLY: HA, LUCID EPISODE INITIALLY AND DETERIORATING IN A FEW HOURS.COMPLICATIONS: BRAIN HERNIATION, CN PALSY. O/A GOOD PROGNOSIS IF QUICKLY EVACUATED.
SUBDURAL HEMATOMA (SDH): RAPTURE OF BRIDGINGVEINS BETWEEN INNER DURA AND THE ARACHNOID.SLOW BUT PROGRESSIVE BLEED. MAY PARTICULARLYAFFECT THE VERY YOUNG AND ELDERLY AND IN ALL AGES (MVA, FALLS ETC.) MAY DEVELOP IN �SHAKEN BABY SYNDROME�. DX MAY BE DELAYED AND WORSEN THE PROGNOSIS WITH HIGH FATALITIES. IN ELDERLY HEAD TRAUMA MAY BE MINOR OR NOT RECALLED. EARLYIMAGING WITH CT IS CRUCIAL. PRESENTS AS CRESCENTSHAPEDCOLLECTION THAT CAN CROSS SUTURES BUT STOPPED AT DURAL REFLECTIONS. DIFFERENTATTENUATION ON CT D/T DIFFERENT STAGES OF BLOODDECOMPOSITION: ACUTE, SUBACUTE,�AND CHRONIC.MAY FORM A CHRONIC COLLECTION-CYSTICHYGROMA. CLINICALLY: VARIABLE PRESENTATION, 45-60% PRESENT WITH SEVERELY DEPRESSED CNS STATUS, PUPILLARY INEQUALITY. OFTEN WITH INITIAL BRAIN CONTUSION, THEN A LUCID EPISODE BEFORE SEVERELYDETERIORATING. IN 30% CASES OF FATAL BRAIN INJURY PATIENTS HAD SDH. RX: URGENT NEUROSURGICAL.
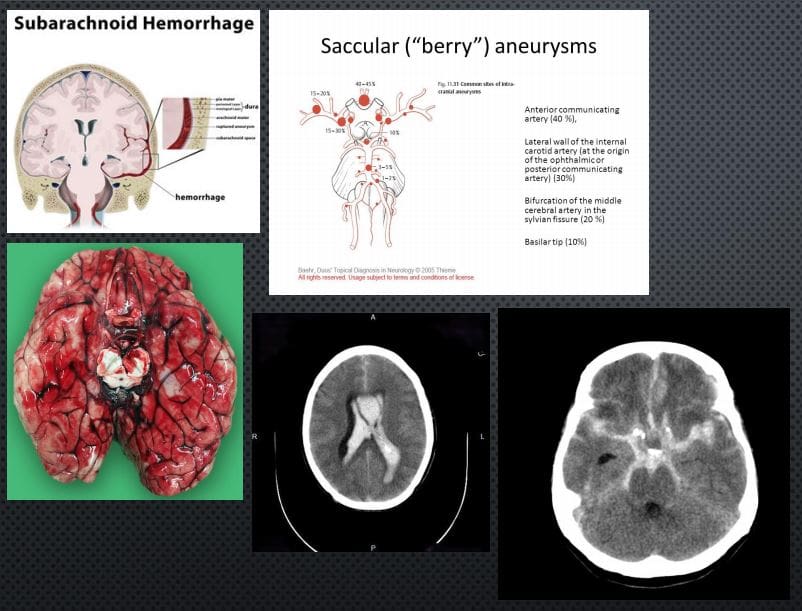
SUBARACHNOID HEMORRHAGE (SAH): BLOOD IN THE SUB-ARACHNOID SPACE AS THE RESULT OF TRAUMATIC OR NON-TRAUMATIC ETIOLOGY: BERRY ANEURYSMS AROUND CIRCLE OF WILLIS.SAH 3% OF STROKES, 5% OF FETAL STROKES.CLINICALLY: PRESENTS AS A �THUNDERCLAP HEADACHE� DESCRIBED AS A �WORST HA INLIFE�. PT COLLAPSES MAY OR MAY NOT REGAIN CONSCIOUSNESS. PATHOGY: DIFFUSE BLOOD INSA SPACE 1)SUPRASELLAR CISTERN WITH DIFFUSE PERIPHERAL EXTENSION, 2)�PERIMESENCEPHALIC, 3) BASAL CISTERNS. BLOOD LEAKED INTO SA SPACE UNDERARTERIAL PRESSURE INDUCES GLOBAL INCREASE IN INTRACRANIAL PRESSURE, ACUTE GLOBAL ISCHEMIA WORSENED BY VASOSPASM AND OTHER CHANGES.
DX: IMAGING: URGENT CT SCANNING W/O CONTRAST, CT ANGIOGRAPHY MAY HELP TO RULE OUT 99% OF SAH. LUMBAR PUNCTUREMAY HELP IN DELAYED PRESENTATION. AFTER INITIAL DX: MR ANGIOGRAPHY HELPS TO FIND THE CAUSE AND OTHER IMPORTANT FEATURES
IMAGING FEATURES: ACUTE BLOOD IS HYPERDENSE ON CT. FOUND IN DIFFERENTCYSTERNS: PERIMESENCEPHALIC, SUPRASELLA, BASAL, VENTRICLES,
RX: INTRAVENOUS ANTIHYPERTENSIVE MEDS, OSMOTIC AGENTS (MANNITOL) TO DECREASEICP. NEUROSURGICAL CLIPPING AND OTHER APPROACHES.
CNS Neoplasms: Benign vs. Malignant
BRAIN TUMORS REPRESENT 2% OF ALL CANCERS. ONE THIRD ARE MALIGNANT, OF WHICH METASTATIC BRAIN LESIONS ARE THE MOST COMMON
CLINICALLY PRESENT WITH LOCAL CNS ABNORMALITIES, INCREASED ICP, INTRACEREBRAL BLEEDING ETC. FAMILIALSYNDROMES: VON-HIPPEL-LANDAU, TUBEROUS SCLEROSIS, TURCOT SYNDROME, NF1 & NF2 INCREASE THE RISK. IN CHILDREN: M/C ASTROCYTOMAS, EPENDYMOMAS, PNETNEOPLASMS (E.G. MEDULLOBLASTOMA) ETC. DX: BASED ON WHO CLASSIFICATION.
IMAGING IS CRUCIAL: INITIAL SYMPTOMS MAY PRESENT AS SEIZURE, ICP SIGNS HA. EVALUATED BY CT AND MRI WITH IV GADOLINIUM.
IMAGING DETERMINES: INTRA-AXIAL VS. EXTRA-AXIALNEOPLASMS. METS FROM PRIMARY BRAIN NEOPLASMS MAYO CCUR VIA CSF AND LOCAL VESSELS INVASION
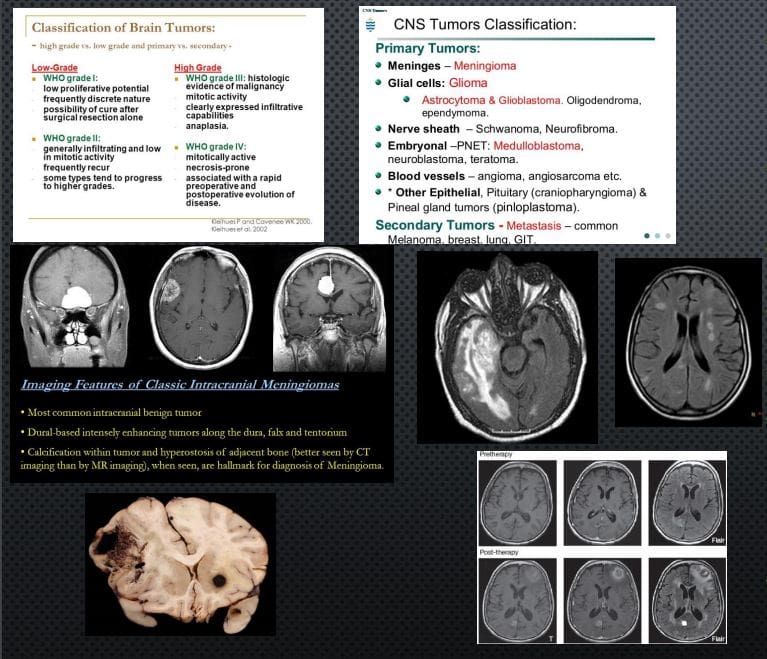
NOTE AXIAL CT SLICE OF MENINGIOMA WITH AVIDCONTRAST ENHANCEMENT.
AXIAL MRI ON FLAIR PULSE SEQUENCE REVEALED EXTENSIVE NEOPLASM AND MARKED CYTOTOXIC EDEMA OF THE BRAIN PARENCHYMA CHARACTERISTIC OF GRADE IV GLIOMA (GBM) WITH VERY POOR PROGNOSIS. ABOVE FAR RIGHT IMAGE: AXIAL MRI FLAIR: BRAIN METASTASIS FROM BREAST CANCER. MELANOMA IS COMMONLY METASTASIZESTO THE BRAIN (SEE PATH SPECIMEN) MRI CAN BE DIAGNOSTIC D/T HIGH SIGNAL ON T1 AND CONTRAST ENHANCEMENT.
RX: NEUROSURGICAL, RADIATION, CHEMOTHERAPY,�IMMUNOTHERAPY TECHNIQUES ARE EMERGING
In all cases, Orthopedic hand surgical referral is required
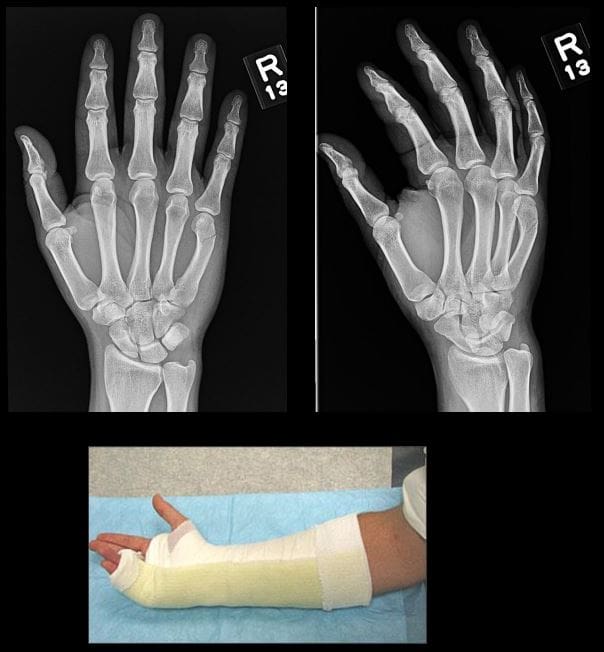
Colles fx: m/c d/t FOOSH+pronation. m/c inOSP/elder women. Rare in men and if occurs need DEXA to avoid hip Fx etc. Young pts: high-energy trauma. Typically extra-articular.50%-cases show Ulna styloid (US) Fx.
Imaging: x-rad is sufficient, CT in complex Fx, MRI helps with ligament tears and TFC.
Rx: if extra-articular and <5-mm distal radius shortening and <5-degree dorsal angulation closed reduction+casting is sufficient. ORIF in complex cases.
�Image Dx: distal rad impaction/shortening,dorsal angulation of distal fragment, carefully examine if intra-articular extension, 50% US Fx
Smith Fx: Goyrand in French literature. Considered as reversed Colles, otherwise almost identical, I.e., 85% extra-articular, 50%US Fx, OSP/elderly women, young pts-high-energy trauma. Differences: mechanismFOOSHwith flexed wrist thus m. Less frequent.
Imaging steps: (see Colles Fx) C
Complications: similar to Colles Fx
Rad Dx: 85% extra-articular with volar(anterior) angulation of the distal fragment,radial shortening. Carefully examine cortical breach suspecting intra-articular extension that can be named as Smith type 2 or Reversed Barton Fx (next)
Rx: similar approach as in Colles.
Barton fx: FOOSH, impaction of distal radius similar to Colles but the Fx line extends from the dorsal radial aspect into radiocarpal joint resulting with dorsal slip/dislocation of the carpus.
Imaging: 1st sept x-radiography often with CTto examine intra-articular Fx extension and operative planning
Rad Dx: distal radius Fx extending from dorsal into the radiocarpal joint with a variable degree of displacement, the proximal slip of the carpus
If Fx line extends from the volar aspect into the wrist joint named Reversed Barton aka Smith type 2 (above bottom image)
Complications: similar to all distal radius Fx
Rx: operative with ORIF
Chauffeur’s/backfire Fx aka Hutchinson Fx: intra-articular Fx of Radial styloid. The name derives from the time when the car had to be started with a hand crank that could backfire inducing wrist dorsiflexion and radial deviation.
Imaging: x-radiography is sufficient. CT may be helpful if Fx not readily shown by x-rays.
Rx: operative with percutaneous lagscrewin all cases d/t intra-articularnature
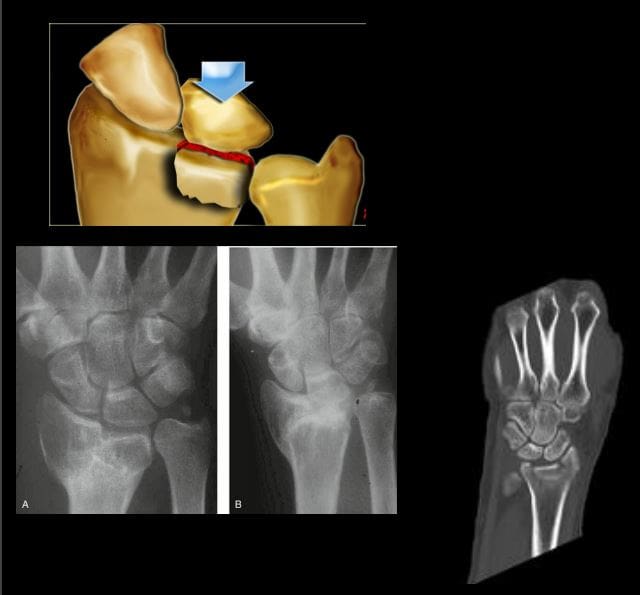
Die-Punch Fx: impaction Fx by the Lunate bone into distal articularLunate fossa of the Radius. IntraarticularFx. Derives its name from a technique to shape (impress) a hole in industrial machining “die-punch.”FOOSH injury.
Imaging: 1st step x-rays, may be equivocal d/t subtle depression of the Lunate fossa then CT scanning is most informative.
Rad Dx: impacted lunate fossa region with intra-articular Fx extension. This can present as a comminuted Fxarticular Fx of the Distal Radius.
Rx: operative d/t intra-articular Fx
Construct arcs of Gilula when evaluating carpal injuries. An Important step required to avoid missing subtle changes in carpal alignment and cortical continuity
Scaphoid bone Fx: m/c Fx carpal bone. D/tFOOSH wrist extended radially deviated. Location of Fx is most important to prognosis: Waist-m/c location (70%). May have 70-100%chance of AVN. Proximal pole Fx: 20-30% with a high risk of non-union. Distal pole-10%shows better prognosis. Distal pole Fx is m/c in children. Key clinical sign; pain in the snuffbox.
Imaging: 1st step-x-radiography but 15-20%missed d/t occult Fx. Special views required. Thus MRI is the most sensitive and specific for early occult Fx. Bone scintigraphy has98/100% specificity & sensitivity esp. 2-3 days after the onset. Key rad. Dx: Fx line if evident, displacement and obscuration of scaphoid(navicular) fat pad, examine for scapholunate dissociation. If proximal bone appears sclerotic-AVN occurred. MRI: low on T1 & high on T2/STIR/FSPD d/t bone edema, a�low signalFx line can be noted.
Rx: Spica cast should be applied if clinically suspected even w/o x-ray findings. For waistFx-cast for 3-mo for prox pole 5-mo immobilization. ORIF or percutaneous pinning with a Herbert screw.
Scapholunate Ligaments Dissociation
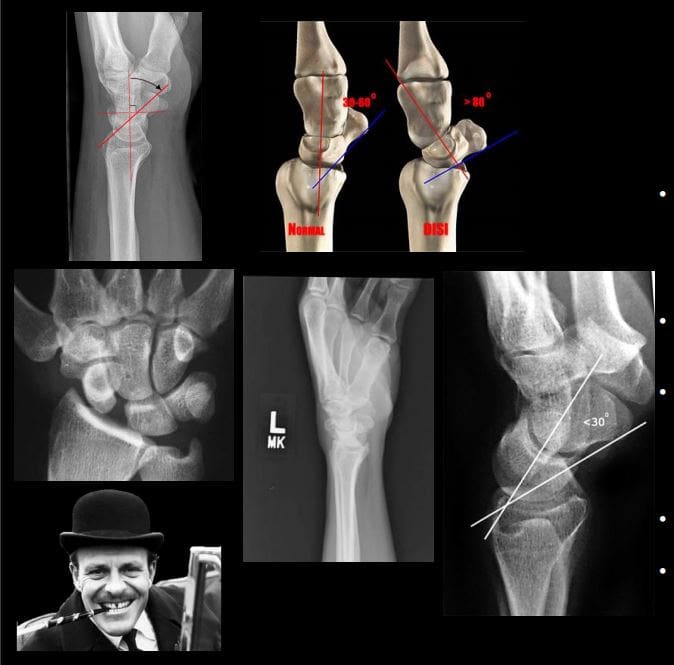
SNAC wrist: scaphoid non-union advanced collapse. Often d/t non-union and dissociation of scapholunate ligaments (SLL)with progressive radiocarpal and intercarpalDJD. The Proximal scaphoid fragment is attached to Lunate with distal dissociating and rotating�signet ring� sign on x-rays.
SNAC wrist may often result in DISI
Rx: progressive DJD may lead to four-corner arthrodesis
Scapholunate advanced collapse (SLAC wrist): SLLdissociation with progressive intercarpal and radiocarpal DJD and volar or dorsal carpal displacement (DISI & VISI). Causes: trauma, CPPD, DJD, Kienboch disease (AVN of Lunate), Preiserdisease (AVN of Scaphoid).
SLL dissociation will lead to Dorsal or VolarIntercarlate aka Intercarpal Segmental Instability (DISIor VISI).
Rad Dx: Dx underlying cause. X-rays demonstrate dorsal or volar angulation of the Lunate with increased or decreased scapholunate angle on the lateral view. On frontal view: Terry Thomas sign or widening of scapholunate distance 3-4-mm as the upper limit of normal.
�MRI may help with ligament evaluation and pre-surgical planning
Rx: often operative with late DJD. Four-corner arthrodesis
Triquetrum Fx: 2nd m/c carpal bone Fx. M/C dorsal aspect is avulsed by the�tough Dorsal radiocarpal ligament. Cause: FOOSH.
Imaging: x-radiography wrist series is sufficient. Best revealed on the lateral view as an avulsed bone fragment adjacent to the dorsum of the Triquetrum. CT may help if radiographically equivocal.
Rx: conservative care
Complications: rare, may persist as pain on the dorsum of the wrist
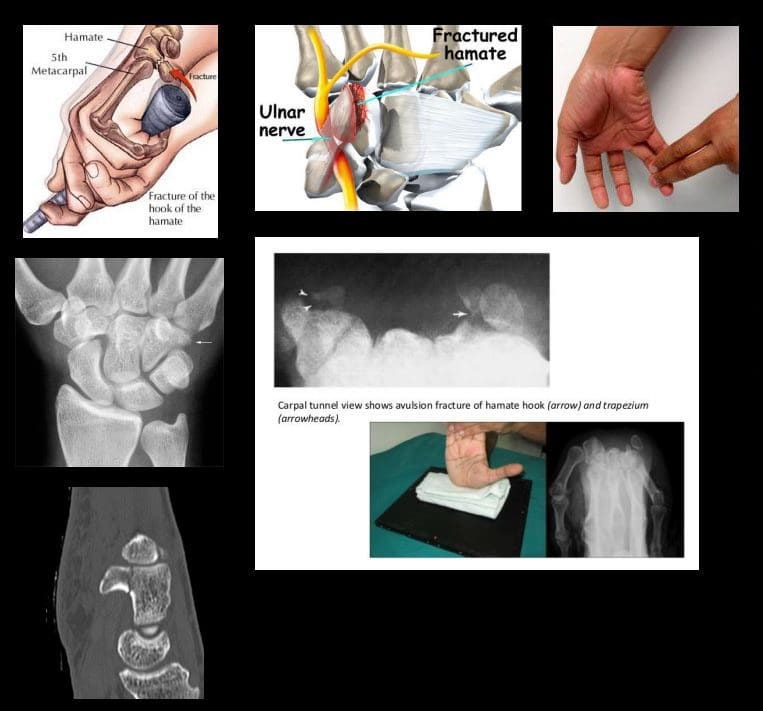
Hook of the Hamate Fx: m/c occurs in batting sports (cricket, baseball, hockey, impact by a golf club, etc.) 2% of carpusFx.
Imaging: x-radiography may fail to detect an Fx unless “carpal tunnel view” is used. CT may help if x-rays unrewarding.
Clinically: pain, positive pull test, weak, painful grip. Deep ulnar n. Branch may be affected within the�Guyon canal.
Rx: usually non-operative, but chronic non-union may require excision.
DDx: bipartite hamate
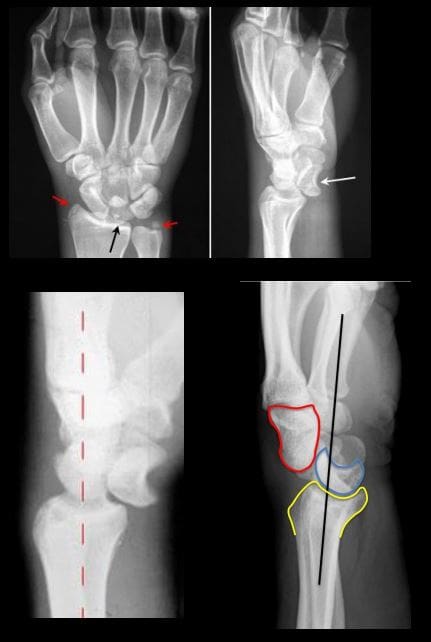
�Lunate vs. Perilunate dislocation: Lunate is m/c dislocated carpal bone. Overall infrequent carpal injury. However, often missed!
Occurs with FOOSH and wrist extended and ulnar deviated. Imaging: 1st step x-rays. Ifunrewarding or require more complex injury evaluation CT scanning.
Key Rad DDx: DDx Lunate from perilunate dislocation. Lunate dislocation: lunate lost its contact with distal radius �spilled teacup� on the lateral. Perilunate dislocation: Lunate maintains its contact with distal radius despite the Capitatedorsally dislocated. Lunate dislocation is additionally helped to identify a �pie sign� d/t Lunate overlapping the Capitate
Rx: emergency reduction and operative repair of torn ligaments
Metacarpal & Phalangeal Injuries
Bennett Fx: intra-articular but noncomminuted impact-type Fx of the base of 1st MC bone of the thumb. X-radiography is sufficient.
Rad Dx: characteristic triangular fragment of bone on the ulnar aspect of the 1st MCbase, often with radial subluxation of the remaining radial aspect of the 1st MC
Complications: DJD, non-union, etc.
Rx: prone to instability/non-union requiring an operative care
Rolando Fx: aka comminuted Bennett with Y or T-configuration. More complex injury. It is unstable requiring operative care
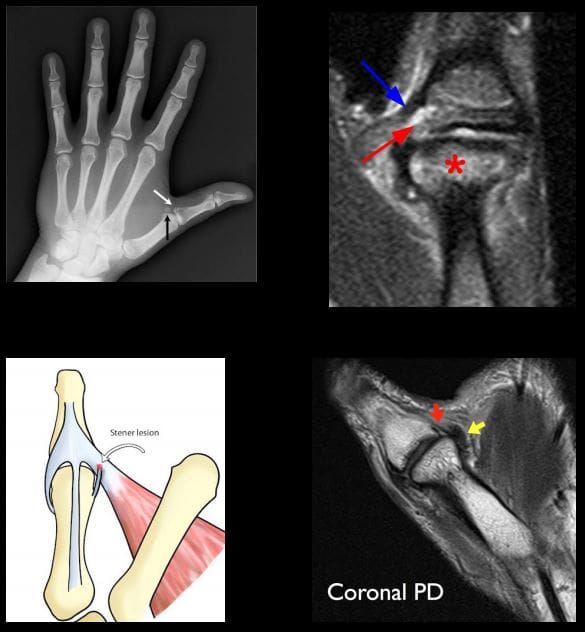
Gamekeeper thumb: traditionally described as a chronic tear of the�ulnar (medial) collateral ligament at 1stMCP in English Gamekeepers’ who performed neck twisting/killing of small game. An acute injury may also be named as Skier’s thumb. This injury can be ligamentous w/o a fracture and an avulsion injury at the 1st proximal phalanx base.
Complication: Stener lesion or displacement of torn ligament over Adductor pollicis muscle that cannot heal w/o surgical repair. MRI Dx is required.
Avoid thumb stress views that can induce a Stenerlesion
Imaging: x-radiography followed by MRI to Dx Stenerlesion. MSK US can be used if MRI is unavailable.
�Stener lesion on MRI & MSUS: ulnar collateral stump is more superficial to Adductor pollicis aponeurosis and appears like a low signal mass-like stump forming so-called “yo-yo on the string sign” reported both on MRI and MSK US.
Rx: often operative
Boxer Fx: m/c MC Fx. An extra-articular usually non-comminuted or minimal comminuted Fx through m/c the 5th and sometimes the 4th MCneck-head junction (occasionally through the shaft) resulting in volar head angulation. Mechanism: direct impact as in clenched fist punching hard surface (e.g., facial bones/wall punching) hence 95% in young males.
Imaging: x-radiography hand series is sufficient
Rad Dx: Fx line transverse or oblique through MCneck with volar head angulation. Evaluate the degree of displacement, critical to report.
N.B. If the same mechanism fractures the 2ndand 3d MC in the same anatomic area, it may require operative care.
Phalangeal hand Fx: m/c skeleton Fx (10% of all Fx). Sports and industrial injuries dominate
Imaging: x-radiography with hand series or PA/lateral finger views will suffice
Rad Dx: if prox phalanx Fx, distal fragment is angled volarly with prox fragment dorsally. Distal phalanx may be angled dorsally. Key observation: nail bed injury, which considered an open Fx with a�risk of infection.
Rx: if <10-degree angulation-buddy-taping with motion rehab. CRPP vs. ORIF can be considered in complex cases-Orthopedic hand surgeon referral
Complication: loss of motion, necrosis, infection.May result with amputation
For additional common injuries: PIP is m/c dislocated joint. Mullet (Baseball) finger, Jersey finger and other injury refer to:
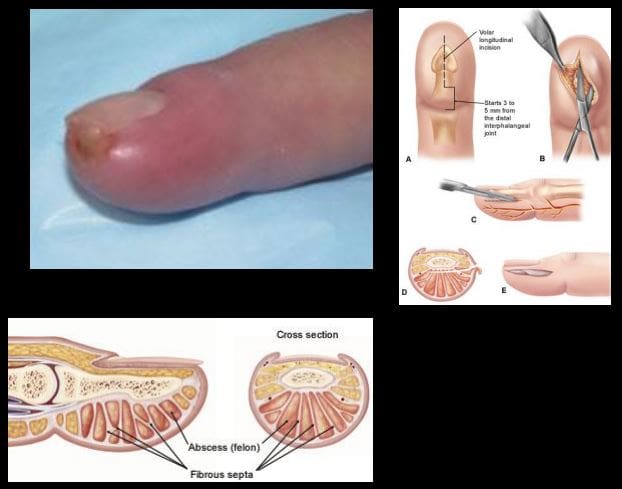
Felon: septic infection of the fingertip pulp typically with Staph.Aureus. Causes: needle prick(diabetics), paronychia, nail splinters, etc. m/c in index and thumb, presenting with pain, swelling, etc.
D/t specific pulp anatomy theinfection>swelling leads to pulp compartment syndrome-pressure and necrosis.
Rx: operative with incision distal to DIP, irrigation/debridement
Pediatric Wrist Injury
Incomplete Fx: Greenstick Fx, Torus (Buckle)Fx, Bowing (Plastic) deformity/Fx. D/t FOSHe.g. fell off the monkey bar. m/c affects <10-years-old.
Rx: usually non-operative (closed reduction and casting)
Distal Radioulnar Joint (DRUJ) Instability-common injury following trauma as in FOOSHwith wrist hyperextension and rotation and disruption of DRUJ ligaments and TFCcomplex. Avulsion of ulnar styloid with the�dorsal or volar displacement of distal ulnar should be noted.
Imaging steps: x-rays initially, MRI may identify ligaments and TFC damage, MSKUScan help with ligaments tearing.
Wrist DJD-typically is secondary to trauma, scapholunate dissociation, SLAC, SNAC wrist, CPPD, Keinboch or Preiser Disease and others.
May lead to major functional loss
Imaging: typically presents as radiocarpal JSL, subchondral sclerosis,osteophytosis, subcortical cysts, and loose bodies. Typically additional induces intercarpal degeneration and particularly Tri-scaphe joint.
MRI may be helpful with early recognition of scapholunate dissociation, Lunate/Navicular AVN.
If isolated MCP OA noted considerCPPD & Hemochromatosis (Hook-like osteophytes)
Clinically:
Mid-age females
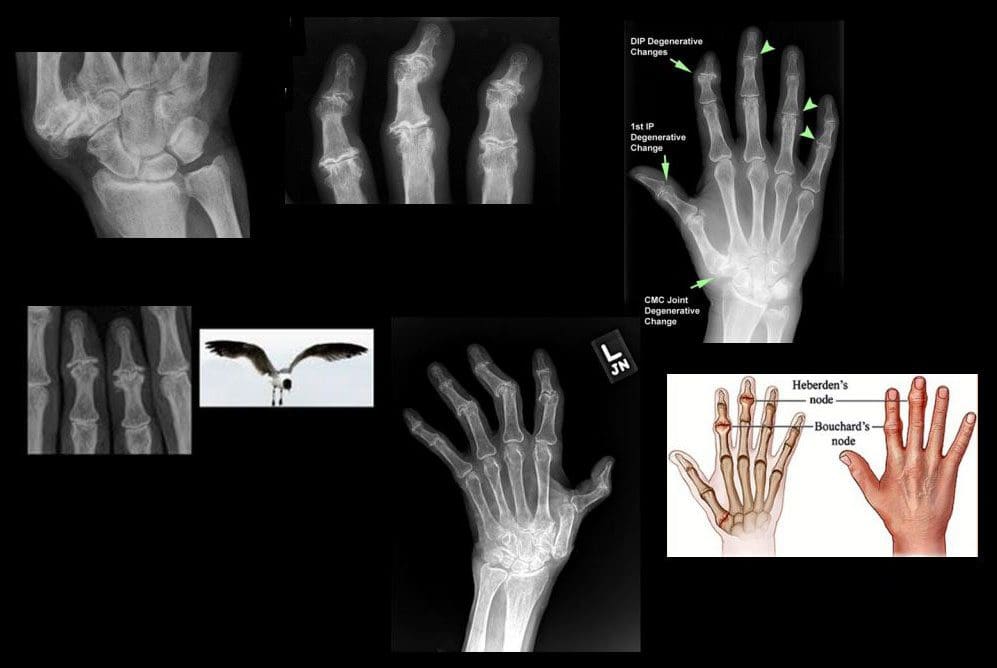
Typically painless except 1st CMC OA
DIPs-Heberden nodes, PIPs-Bouchard nodes
Erosive OA (occasionally called�inflammatory OA�)
A Spectrum of OA but producing central proximal erosions at DIPs and PIPsresulting with very characteristic �gullwing� appearance. No systemic inflammation (no CRP, RF, Anti-CCP Ab)typically in middle-aged/elderly females, like Hand OA, often seen in families
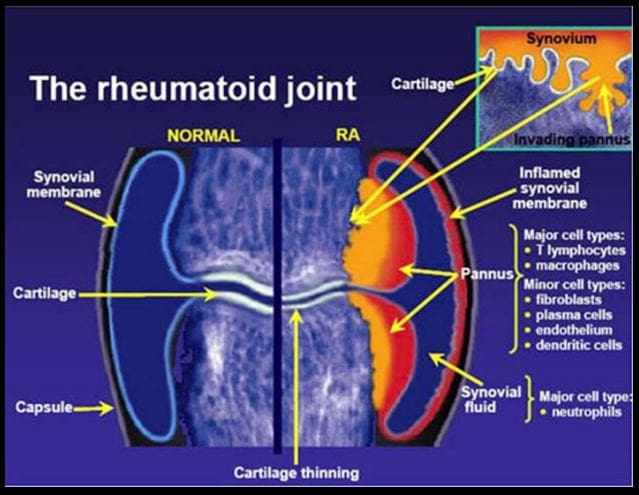
Rheumatoid Arthritis
Rheumatoid Arthritis (RA)-chronic systemic inflammatory disease of unknown etiology, targeting synovial joints, tendons with multiple systemic involvement (lung, CVS, Ocular, Skin, etc.) Pathology: Tcell>Macrophage/APC>mediatedautoimmune process resulting in pannus formation and gradual destruction of ST, cartilage, bone,�and other tissues. 3% FemalesVS.1% Males. Environmental triggers: infection, trauma, smoking,�and others in a genetically susceptible individual. 20-30%may be disabled after 10-years.
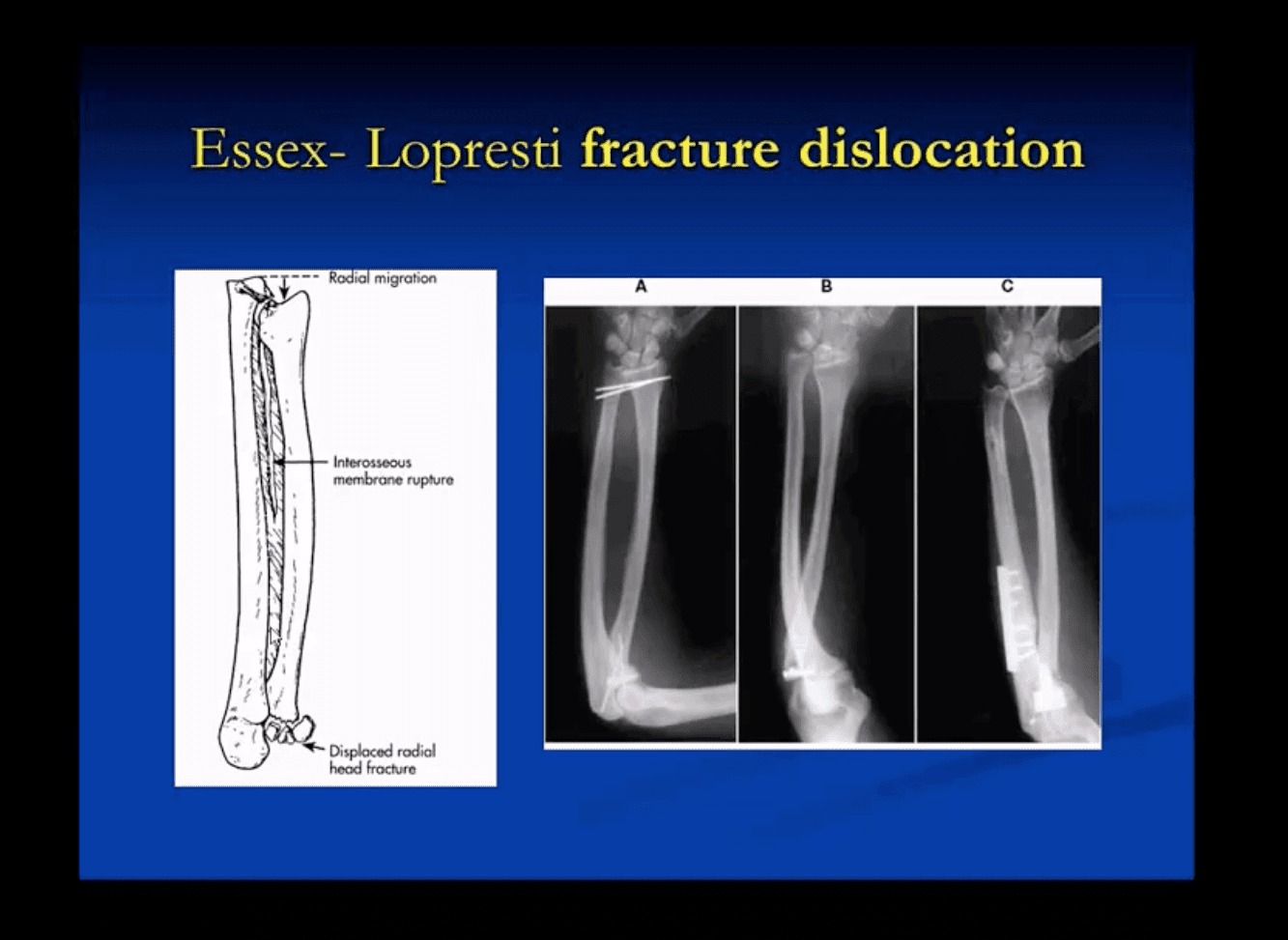
In adults: Radial head Fx is the m/c (33%) and accounts for 1.5-4% of all fractures. Etiology: FOOSH with forearm pronated. Associated injuries: elbow collateral ligaments tears. EssexLoprestiFx with interosseous membrane tearing and dislocation of the Distal Radio-Ulnar Joint(DRUJ)
Terrible triad: of the Radial head Fx, elbow dislocation and Coronoid process Fx (typically avulsed by the Brachialis M)
Imaging: 1st step is x-radiography with elbow series, CT scanning may help in complex cases, MRIif ligamentous injury.
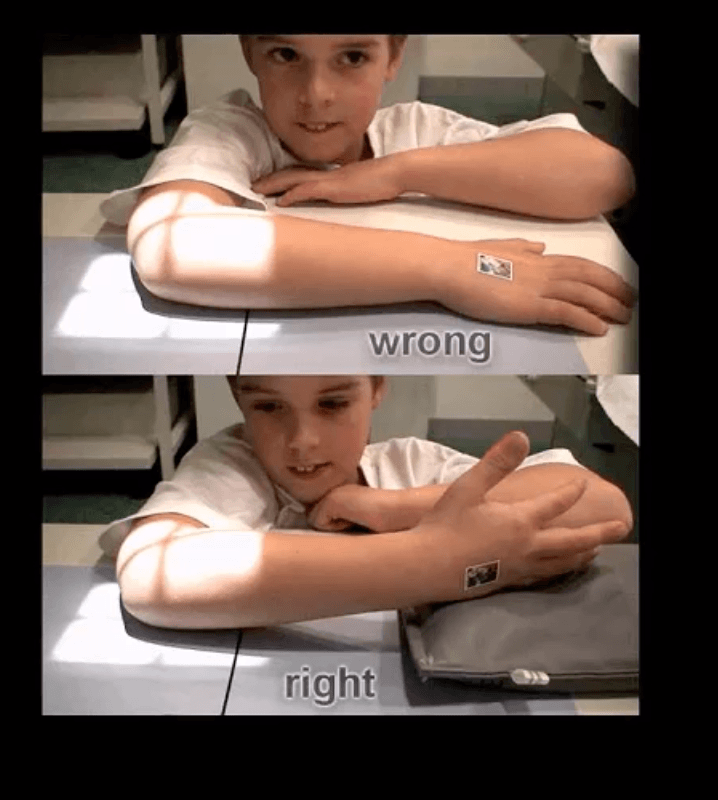
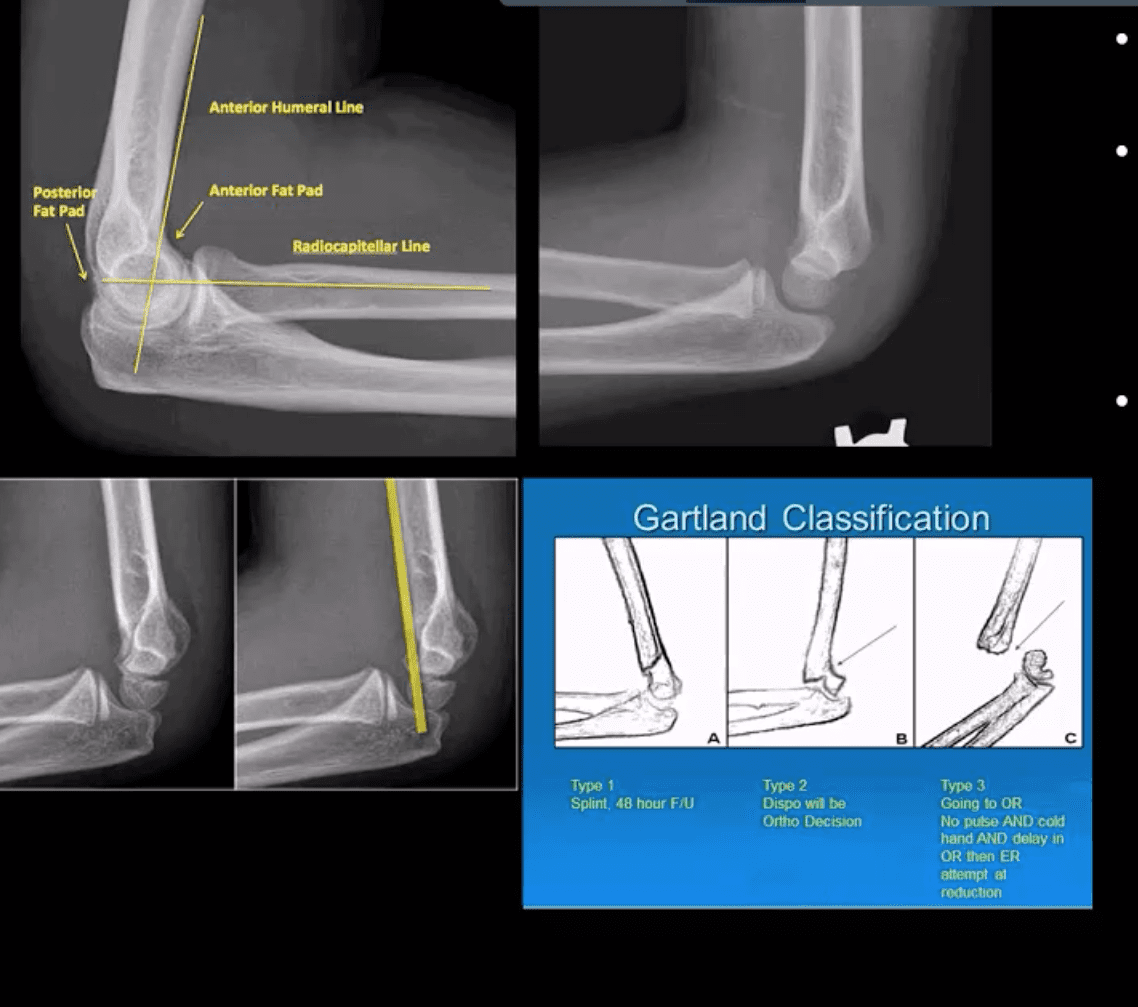
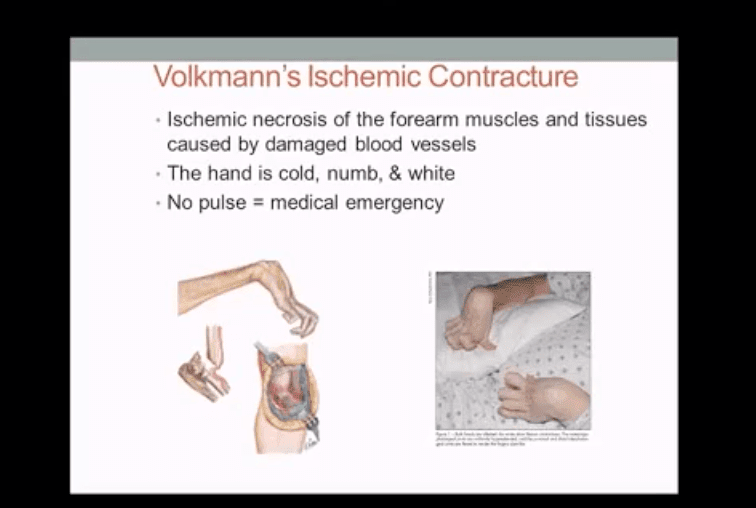
In children: Supracondylar Fx of the distal humerus accounts for 90% of acute trauma. It is always d/t accidental trauma with FOOSH and elbow extended, rarely <5% with flexed elbow. MostSupracondylar Fx occur in children <10 y.o. Males>Females. Complications: malunion in cubitus varus aka Gunstock deformity, vascular injury and acute ischemic compartment syndrome with Volkmann contracture
Imaging: 1st step x-radiography can be sufficient. CT occasionally used in complex cases.
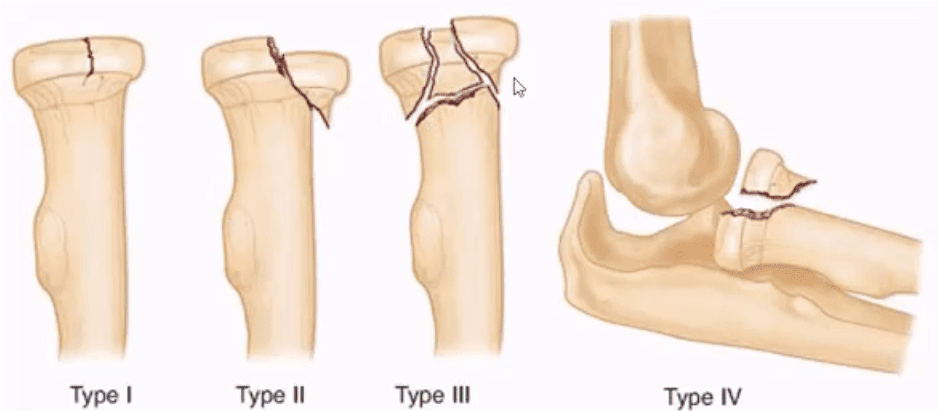
Radial head (RH) Fx: Mason classification helps to determine the degree of complexity and mode of treatment
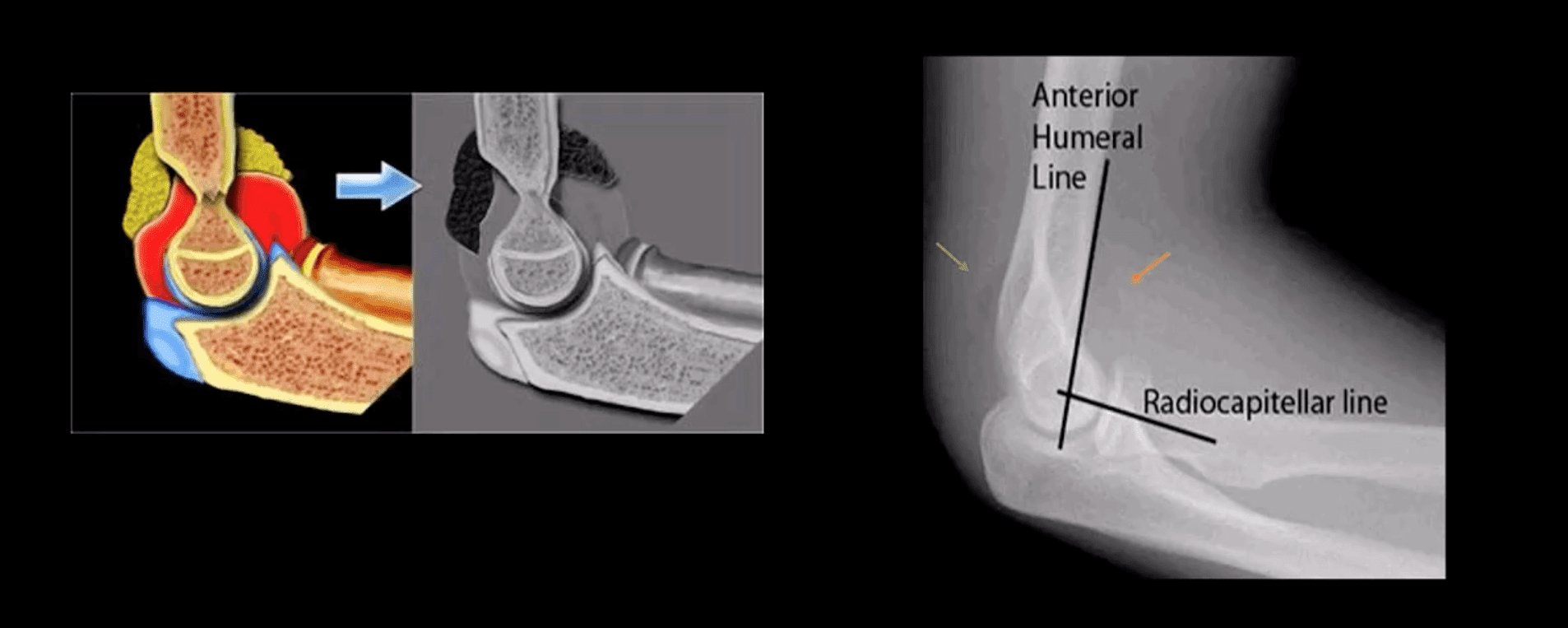
Type 1- undisplaced is the m/c and stable contained by ligaments. On radiographs can be very subtle and evaluation of abnormal elbow fat pads is critical and often the only diagnostic clue
Type 2- displaced by 2-mm or > with rotational block
Type 3- comminuted >2-3 fragments and
Type4 is presented with RH fx, posterior elbow dislocation and sometimes Coronoid process fracture often d/t Brachialis M avulsion
Rx: Type 1 managed non-operatively by immobilization and movement rehab. Type 2- ORIF if rotational block. Type 3 and 4, ORIF and RH resection or RH arthroplasty
Note abnormally displaced anterior fat pad (orange arrow) and the emergence of the posterior fat pad (green arrow) that is usually deep in the olecranon fossa and not seen unless acute hemarthrosis or other effusiondevelopsFat pad signs are most reliable indicators of intra-articular elbow Fx
Mason type 1 RH Fx can be v. subtle and missed. Radiographic search should involve a�close evaluation of positive fat pad signs. Note anterior fat pad displacement aka Sail sign and the presence of the post fat pad d/t acute bleed
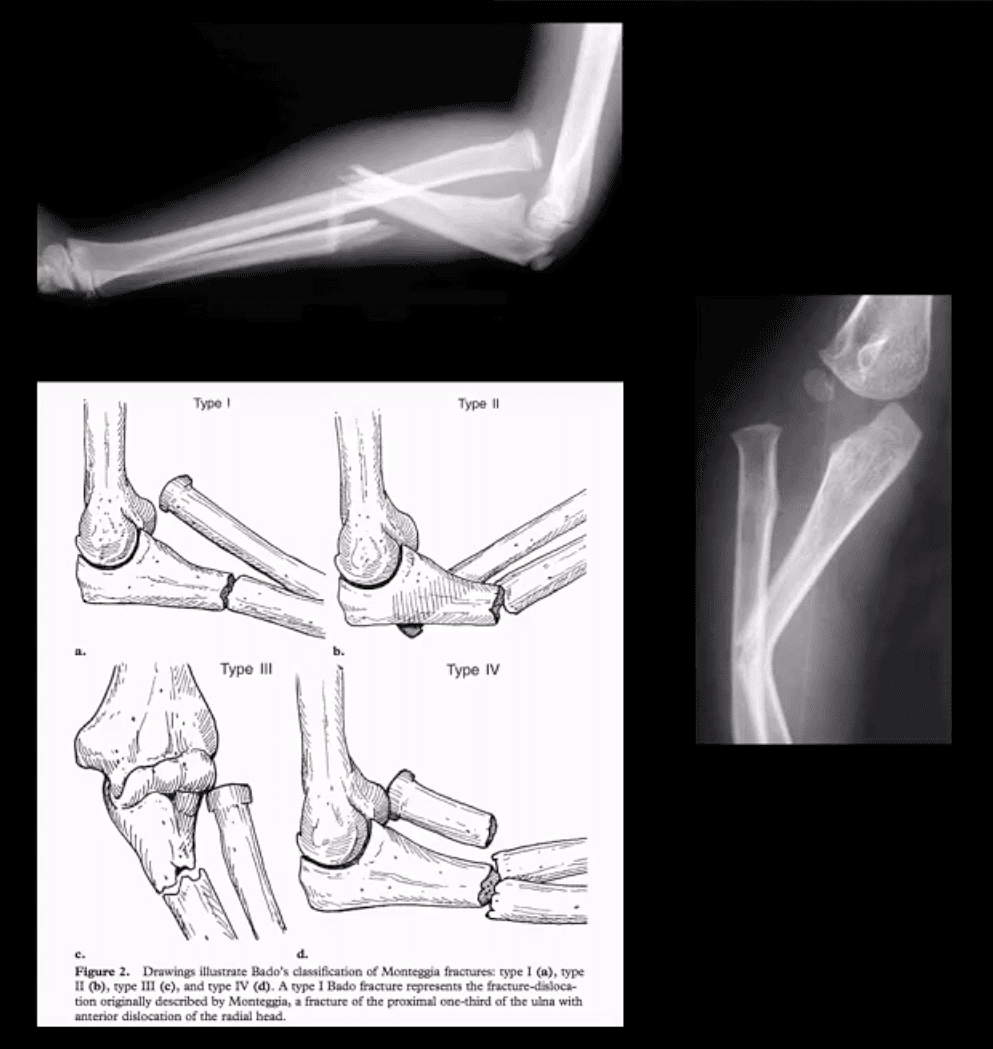
Monteggia fracture-dislocations: prox 1/3ulnar shaft Fx. with concomitant dislocation of PRUJ (radial head). FOOSH injury. Children4-12 y.o. Infrequent in adults.
X-rays readily reveal ulnar Fx, but radial head dislocation may be subtle and occasionally missed. This is a serious injury leading to elbow disability if Dx delayed 2-3 weeks or left untreated. X-rays are typically sufficient:Rx: casting vs. operative.
Supracondylar Fx: this is the M/C elbow Fx in children.
Especially, the un-displaced types 1(top right) is difficult to Dx. Abnormality of “fat pads” and anterior humeral line and radiocapitella line disturbance are often most reliable
Type 3 carries a particularly high risk for Volkmann contracture (vascular ischemic-necrosis of the anterior forearm muscle compartment
Elbow complaints in a young athlete
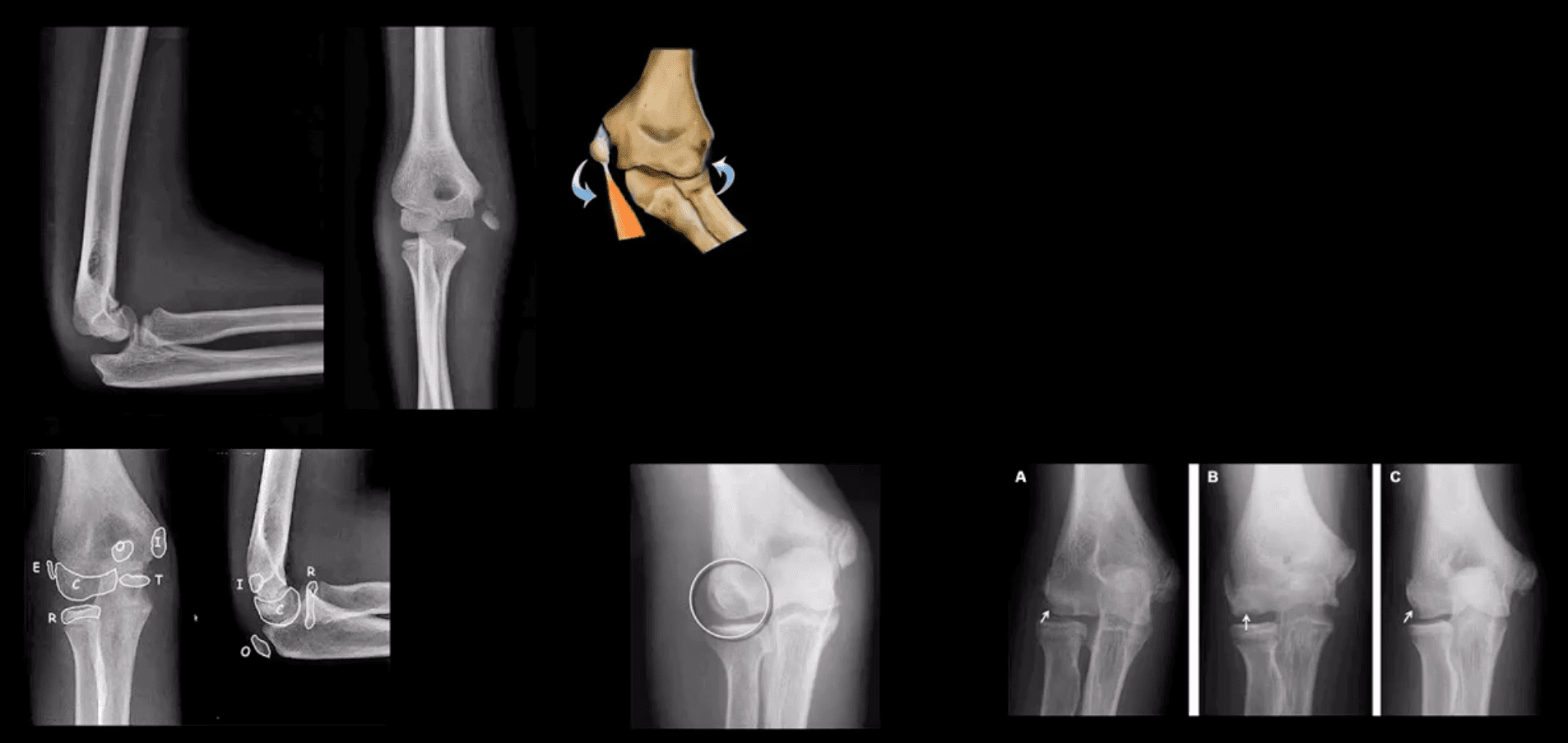
Epicondyle Fx: common pediatric injury, about 10%.Essentially an avulsion Fx and a MUCL tear. Medial epicondyle is m/c Fx. FOOSH is the m/c mechanism.M>F. If minimally displaced or undisplaced can be treated with casting esp. in non-dominant arm. If displaced as in this case, require ORIF.
Medial epicondyle avulsive Fx in a young baseball pitcher was coined a �little league elbow� in the 60sand now should be avoided to avoid confusion
OCD of the Capitellum is a common athletic injury induced by repeated compression/flexion. OCD must be DDx from Panner�s disease or osteochondritis typically presented in younger patients
Difficulty in diagnosis may stem�from multipleapophysis about the elbow (see CRITOE)
Imaging: 1st step: x-rays followed by MRI and MRarthrogramme if indicated.
CT may help with complex injury evaluation. MRI and MSKUS may help with a�ligament injury.
Elbow Arthritis
DJD of the elbow is uncommon and typically 2nd to trauma, occupation, CPPD, OCD of theCapitellum or other pathology. Clinically: pain, reduced ROM esp. in dominant arm, deterioration of ADL. Loss of terminal flexion and extension. 50% develop Ulnarcompressive neuropathy. Rx: conservative,arthroscopic debridement/osteophytes removal, capsular release. In older patients and not active patients Total Elbow Arthroplasty (TEA) can be used
Imaging: x-radiography is sufficient, CT helps with pre-operative planning
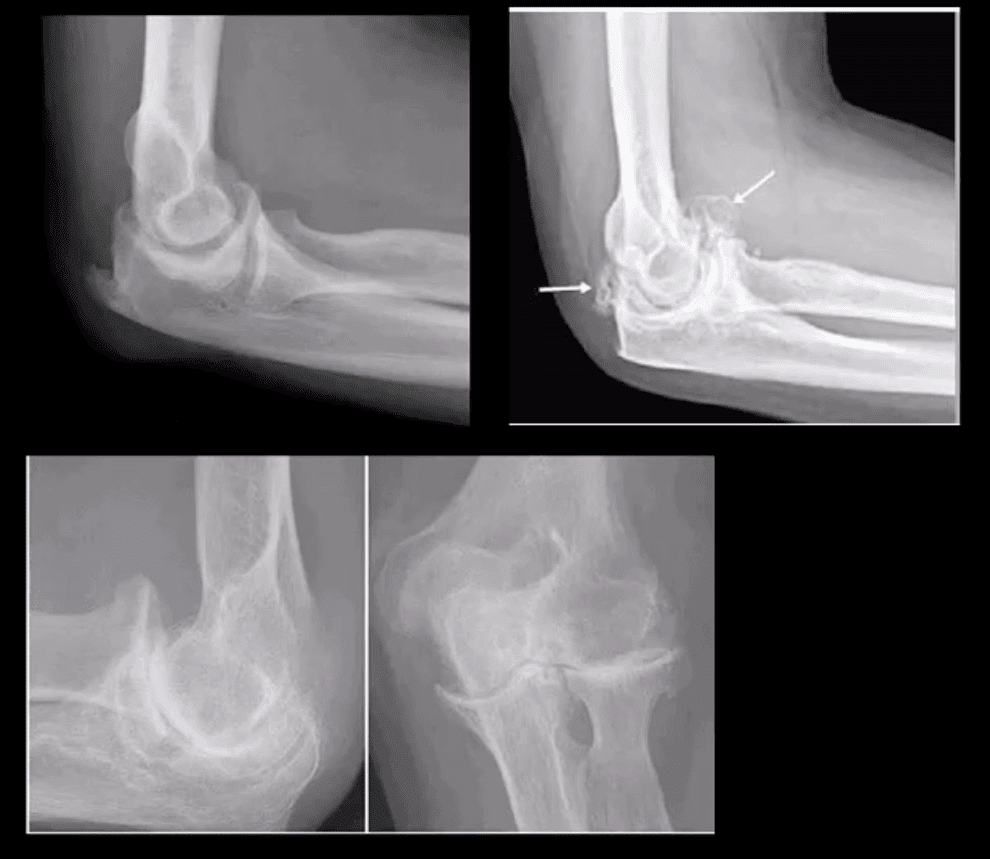
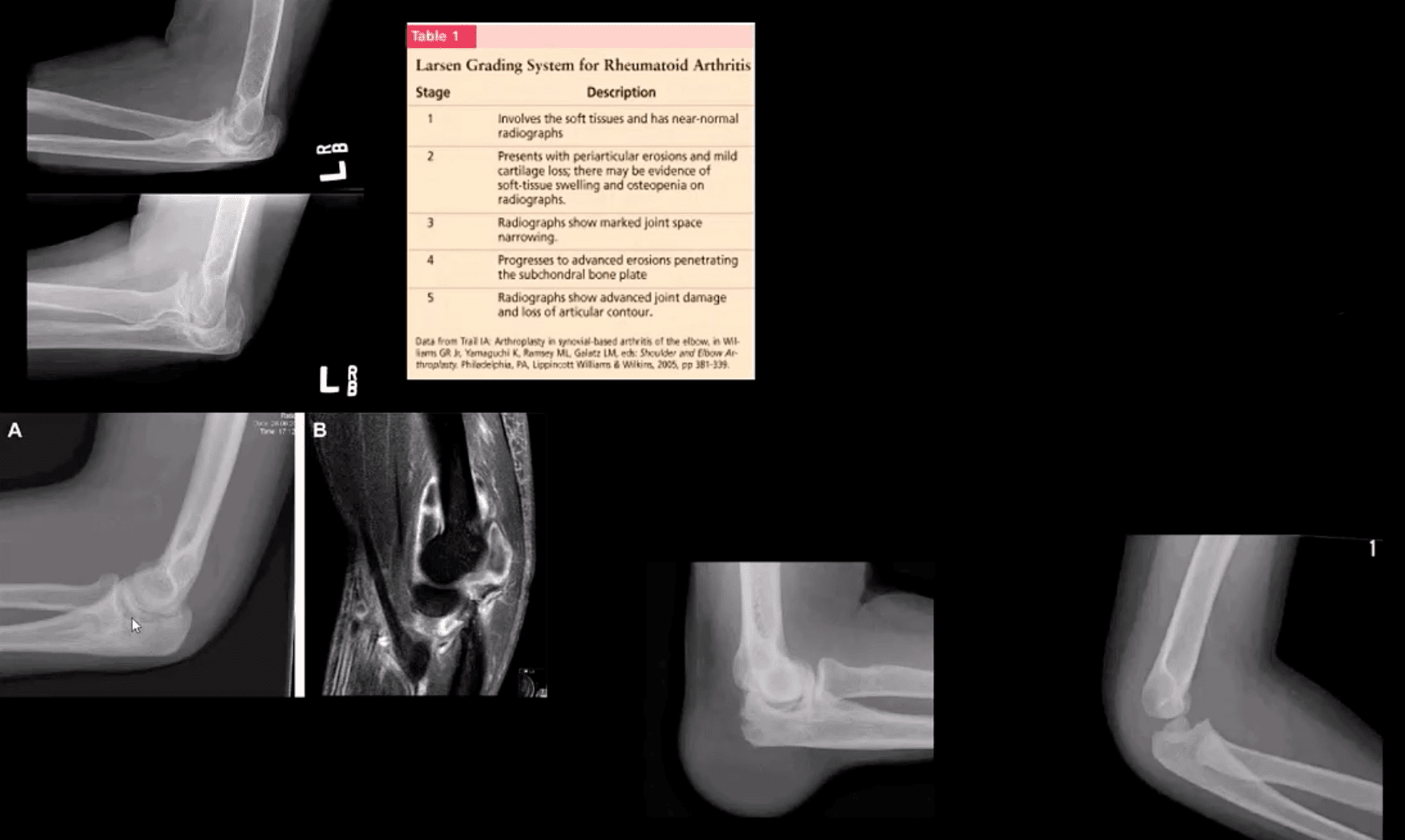
Inflammatory Arthritis: RA of the elbow is frequent (20-50%) and destructive d/t synovitis, pannus, bone/cartilage,�and ligamentous destruction/laxity. Clinically: begins after the onset of hands symptoms with, symmetrical swelling, pain, reduced ROM, flexion contracture. Presence of rheumatoid nodules can be noted along the olecranon and posterior forearm. Rx: DMARD, operative tendons repair.
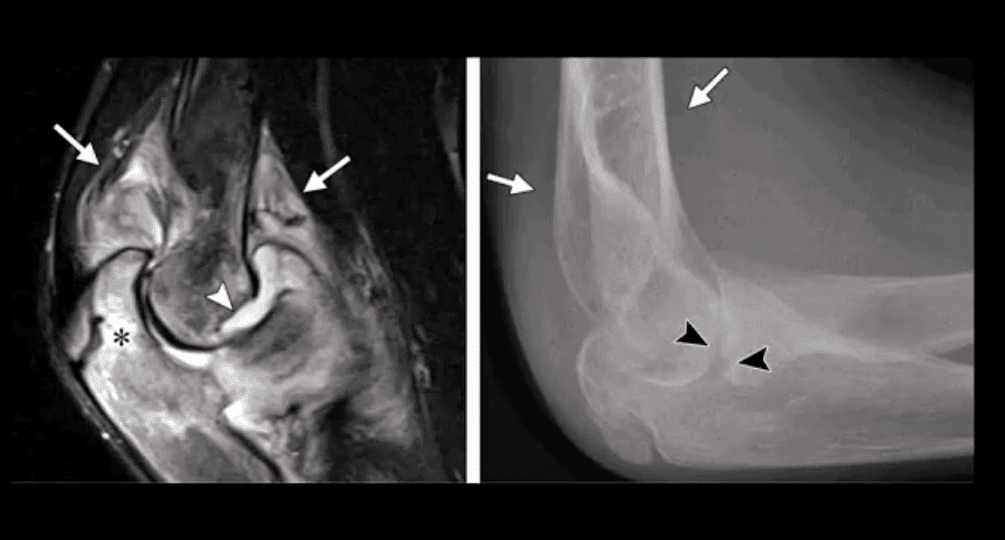
Imaging: x-radiography with early non-specific effusion (fat pads),later: erosions, symmetric JSL, osteopenia. MSK US helps early Dx. MRI reveals synovitis; bone edema correlates with pre-erosive x-ray findings, synovial enhancement on FS T1+C.
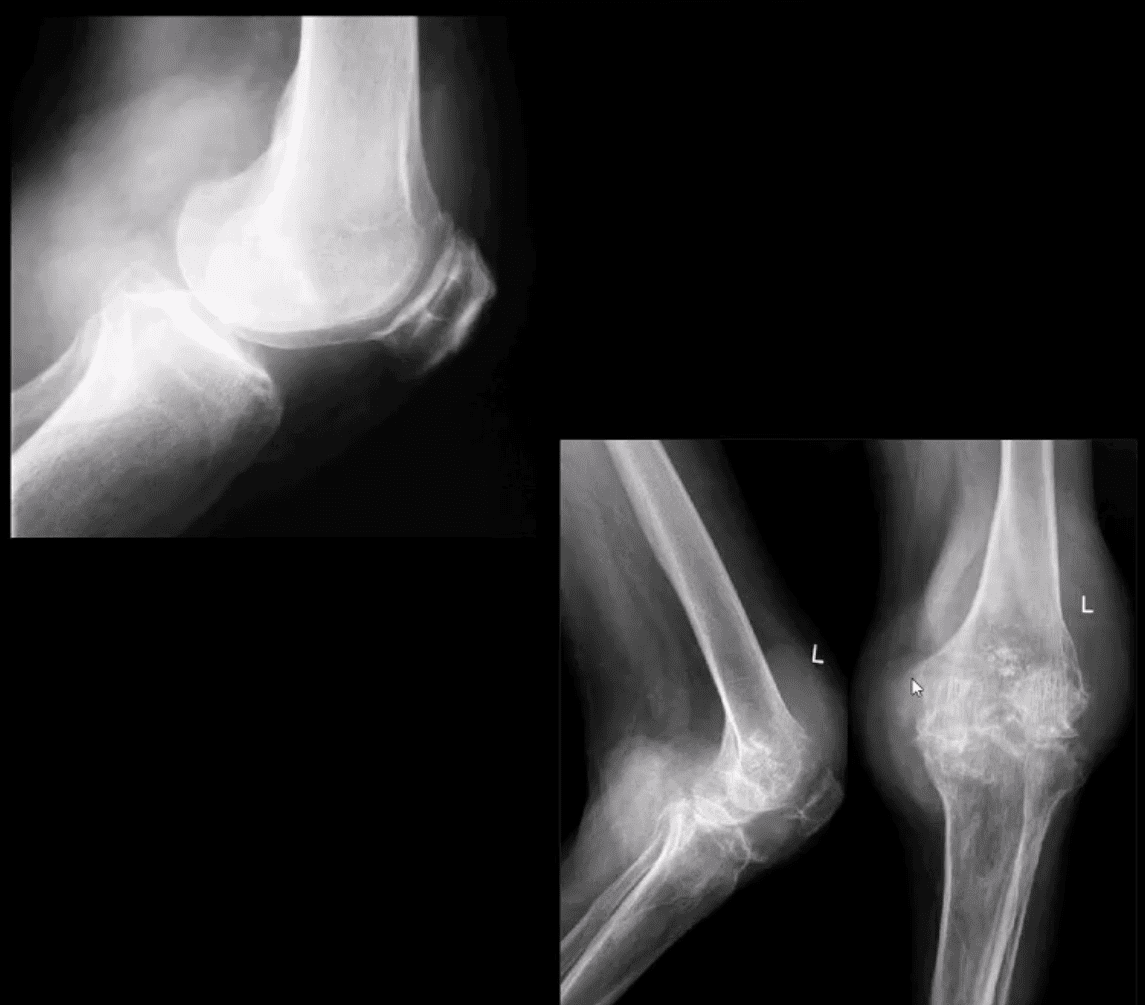
Gouty Arthritis: may affect the elbow but less than in the lower extremity. Olecranon bursitis causing a �rising sun sign� on x-rays with or w/o bone erosions. Aspiration and polarised microscopy revealing needle-shaped negatively birefringent monosodium urate crystals. Rx: colchicine, other meds.
Septic Arthritis: consider in people with diabetes, IV drug users, concurrent RA, patients with active TB, gonococcal in young adults. Clinically presents as monoarthritis with or w/o constitutional signs. X-ray: poor detection in early stages. US may show effusion and high Doppler.MRI: effusion, osseous edema. Bone scintigraphy can help as well. Labs: CBC, ESR, CRP. Diagnostic arthrocentesis with gram staining and culture are crucial. Rx: Prompt IV antibiotics
Juvenile Idiopathic Arthritis (JIA) considered M/C chronic disease of childhood and preceded IBD infrequency. Dx is clinical and imaging: Criteria: Joint pain and swelling in a child 0-16-years for 6-weeks or longer. Many forms exist�M/C pauciarticular(oligoarticular) 40%, F>M, associated with ocular involvement (iridocyclitis) and potential blindness. Polyarticular and Systemic forms.
Elbow is frequently affected along with the knee, wrists,�and hands,�especially in polyarticular dz.
Labs: ESR/CRP RF-VE in most cases
Imaging: early x-ray features are non-specific. Later: osseous erosion, destruction of joint cartilage, overgrowth of articular epiphyses, early closure of physis. Delayed features: 2nd DJD, joint ankyloses.DDx: hemophilic arthropathy. Cervical radiographs are crucial.
Rx: DMARD, conservative care
Miscellaneous pathologies
Supracondylar process: 2% of the population. Described by Sir JohnStruthers in 1854. Fibrous band(Ligament of Struthers) may lead to compression of the Median N. DDx fromOsteochondroma that typically points away from the joint
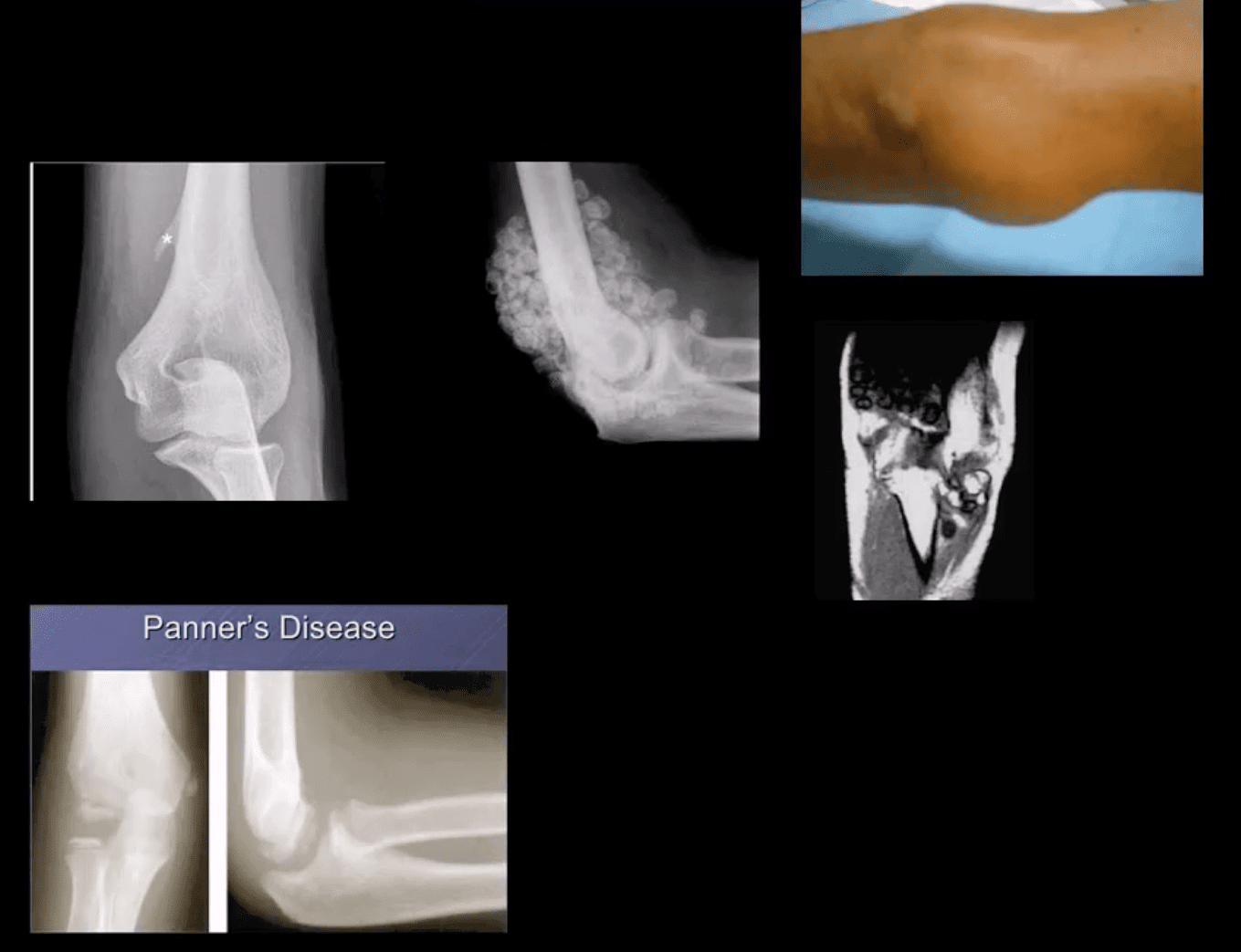
Primary synovial chondrometaplasia�(Reichel Syndrome): abnormalmetaplasia of synovial cells shedding cartilage into joint potentially causing DJD, extrinsic bone erosion, synovitis, nerve compressions etc. Removedoperatively. Imaging: multiple osseocartilaginous loose bodies of relatively equal sizes in the joint cavityDDx with DJD and 2ndosteochondromatosis. MRI-low signal onT1 and T2 with potential joint effusion. Ina tight joint like the elbow may present with large joint distention.�
Panner�s Disease: osteochondrosis of theCapitellum typically in 5-10 y.o. young athlete DDX from OCD of Capitellum(discussed) that occurs in teenagers.Clinically: pain on activity. Recovery occurs in most cases by spontaneous healing. Imaging: x-rays reveal sclerosis and slight fragmentation of theCapitellum w/o loose body. MRI: low T1and high T2 signal in the entireCapitellum.
Myositis Ossificance:
Soft Tissue & Bone Neoplasms about the Elbow
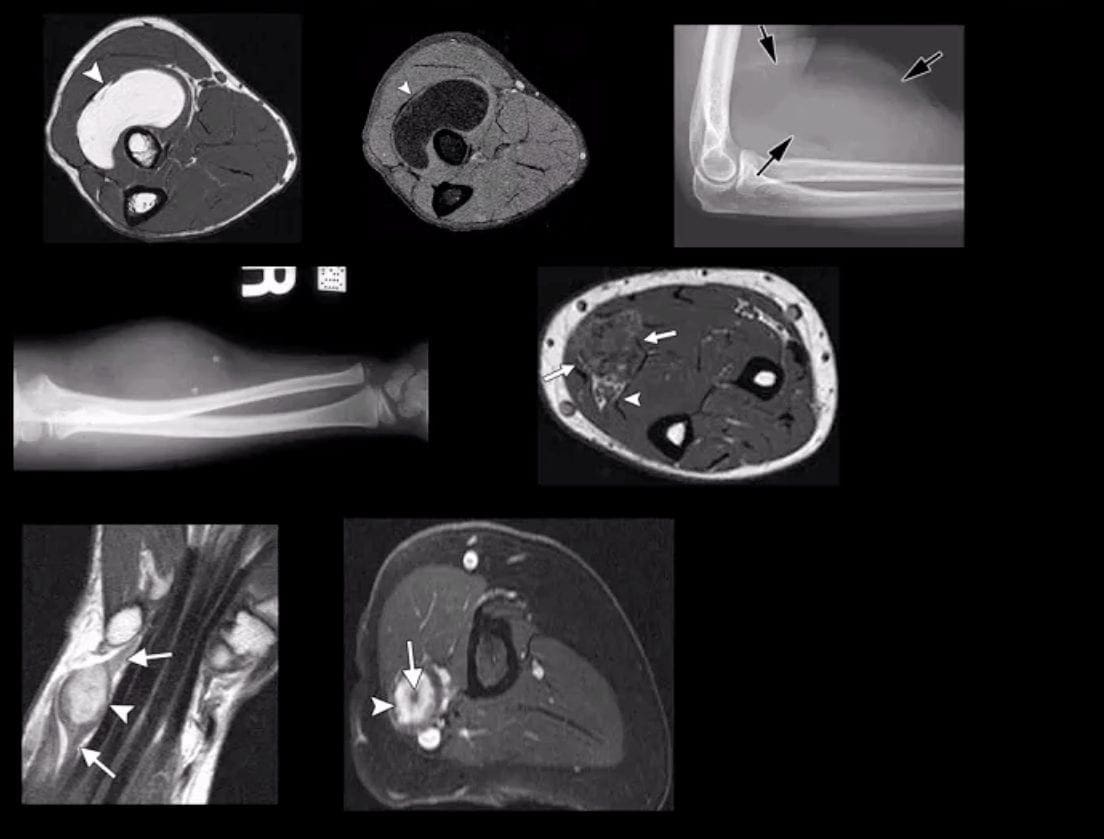
Lipoma: intramuscular, subcutaneous. Most common soft tissue neoplasms. Composed of fat but a substantial number may undergo fat necrosis-calcification-fibrosis. Typically remains benign. Occasionally difficult to DDx from a well-differentiated liposarcoma. Imaging: x radiography: radiolucent lesion well-circumscribed with or w/o calcification. US and MRI are important. On MRIT1high, T2 low SI.
Hemangioma: benign vascular lesion, often composed of multiple vascular channels. Capillary vs. cavernous. More common in children, but found in any age. May often form phleboliths (calcification). Imaging: x-rays reveal soft tissue mass containing phleboliths. MRI: T1-high or variable signal. T2-high signal in areas of slow flow. �bag of worms� sign. Biopsy best avoided. Rx: difficult: local excision vs. embolization vs. observation. High recurrence.
Peripheral Nerve sheath tumor (PNST): benign vs.malignant. Greater incidence in NF1 with a higher risk of malignant PNST. Benign PNST: Schwannoma vs.Neurofibroma. Spinal vs. peripheral nerves. Histology: Schwann cells interspersed with fibroblast and vessels.Clinically: pts in 20s and 30s, palpable mass with or w/o local pressure. Imaging: MRI: T1: split-fat sign, T2: target sign. T1+C enhancement
Soft Tissue Sarcomas: MFH, Synovial sarcoma,(discussed), Liposarcoma (more frequent in the retroperitoneum) Dx: MRI. Clinically: Dx is delayed d/t painless enlarging mass often ignored. Clinically palpable mass deserves MRI examination, US may be helpful. Biopsy confirms Dx.
Malignant bone Neoplasms: Children: OSA, Ewing�s sarcoma (discussed) Adults: Mets, Myeloma (discussed)
Proximal humeral Fx account for 4-6% of all Fxs. Osteoporotic (OSP) Fx in >60 y.o associated with minimal trauma with F: M 2:1 ratio. In young patients, acute high energy trauma predominates.
Complications: AVN humeral head, Axillary N paralysis.
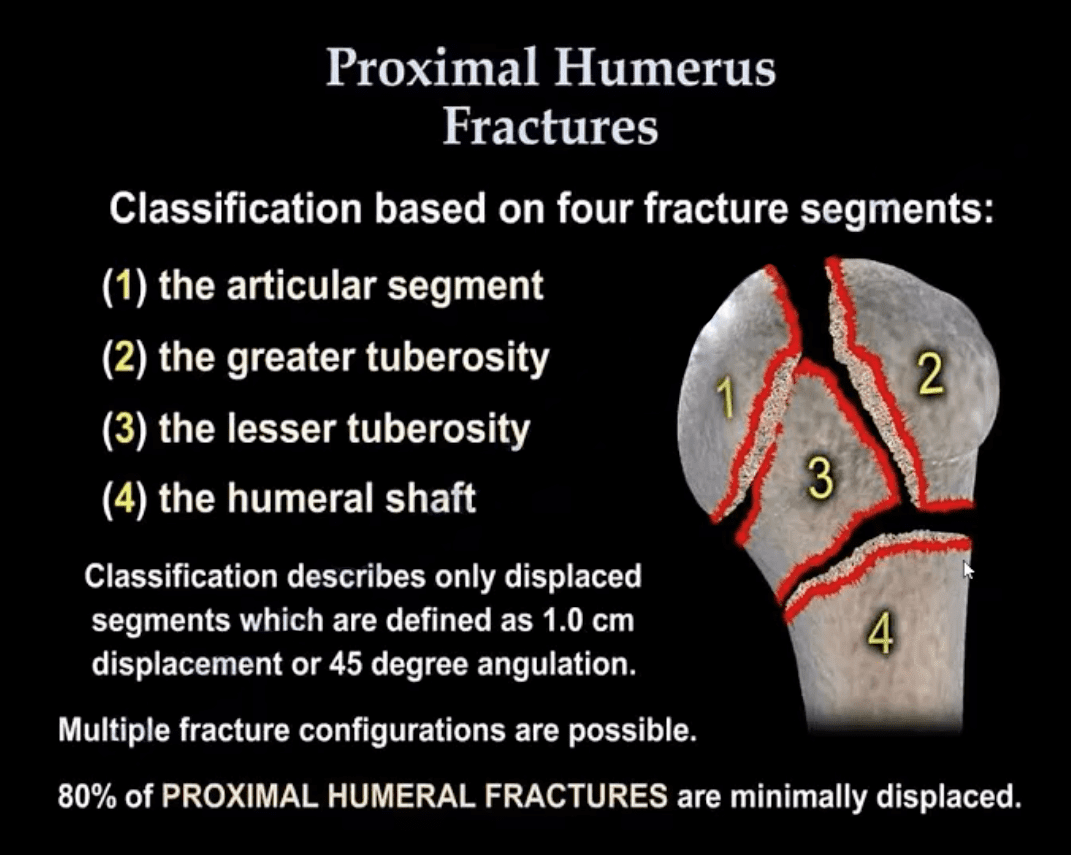
Neer Classification: considers fractures along 4-anatomical lines with or w/o displacement >1-cm & 45-degree angulation
One part Neer Fx- no displacement or very minimal <1-cm/45-degree. Can affect 1-4 lines and M/C at greater tuberosity. 80% of proximal humeral Fx are one-part Neer.
Two-part Fx: 1-part is displaced >1-cm/45-degrees. m/c involves the surgical neck
Three-part Fx: 2-parts are displaced >1-cm/45-degrees.
Four-part Fx: all 4-parts can be displaced. Uncommon <1%
Imaging: 1st step-radiography, CT may be used in more complex cases. Orthopedic referral
Management: Neer one-part Fx is treated with Sling Immobilisation and progressive rehab
The vast majority of Fx in the elderly are treated non-operatively
Younger patients (40-65) may occasionally require hemiarthroplasty if 3 or 4-part Neer Fx present. Greater risk of AVN
Proximal Humerus Fractures
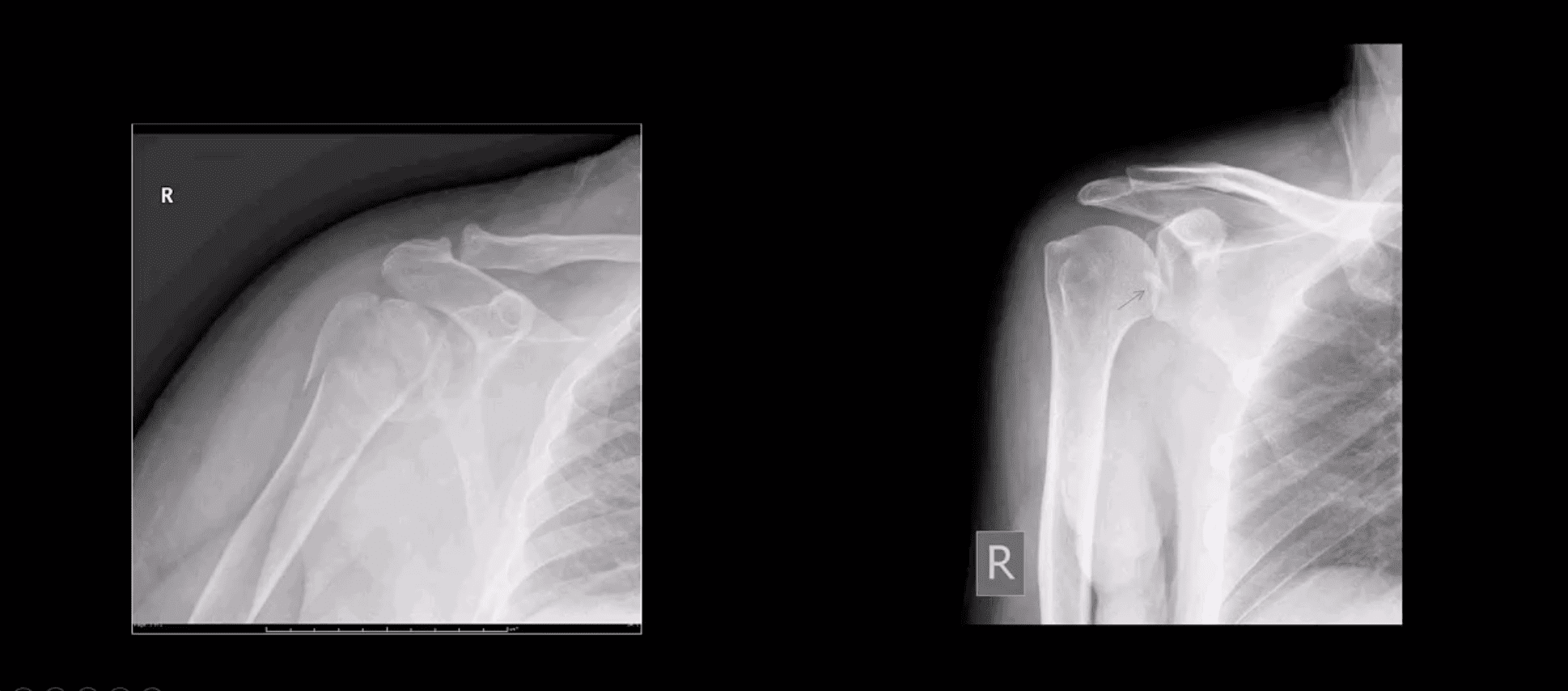
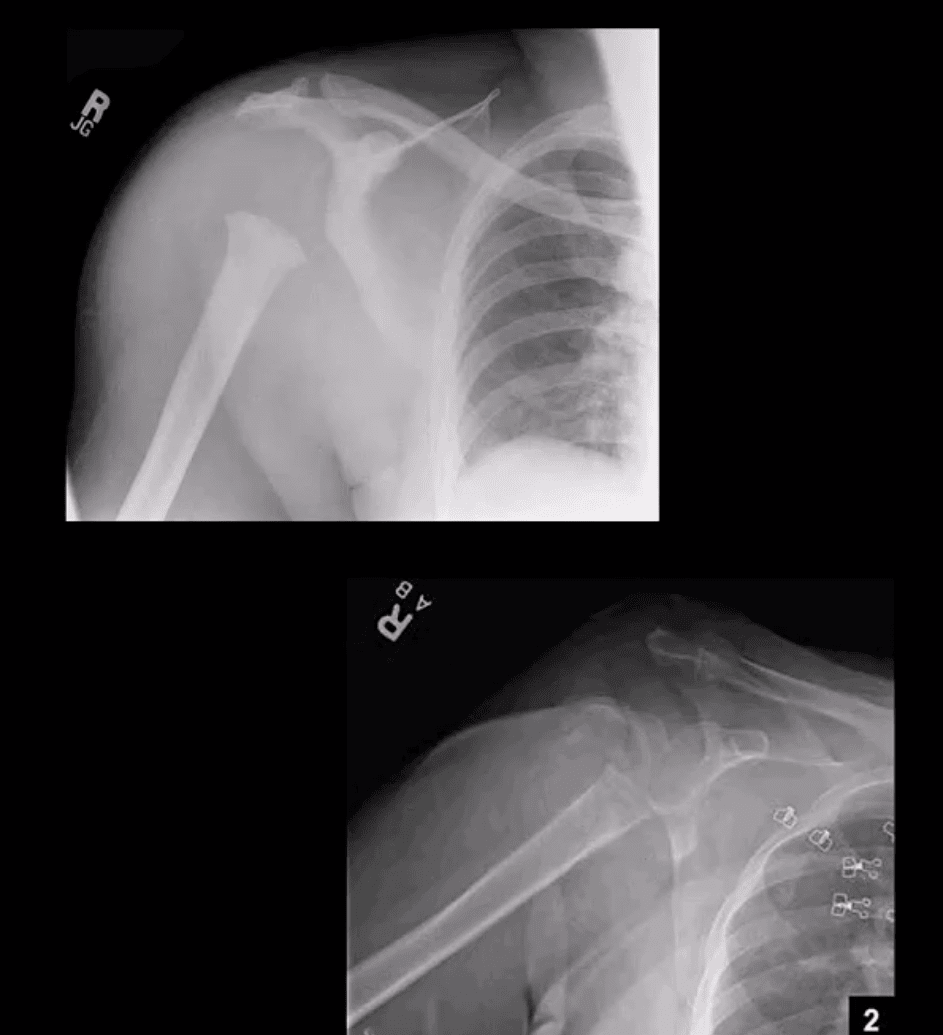
Note: Left image: Fx involving the anatomical neck and the greater tuberosity with minimal displacement <1-cm/45-degree thus Dx as one-part Fx. Right image: Small avulsion Fx of the greater tuberosity with significant displacement (>45-degrees & 1-cm) thus Dx as two-part Fx
Note: three-part Neer Fx (left) and four-part Neer Fx (right)> Management: operative in most cases in younger (40-65) patients
Refers to complete separation of the humerus from scapula glenoid. In 20-40s M: F 9:1 ratio, in60-80S M: F 3:1
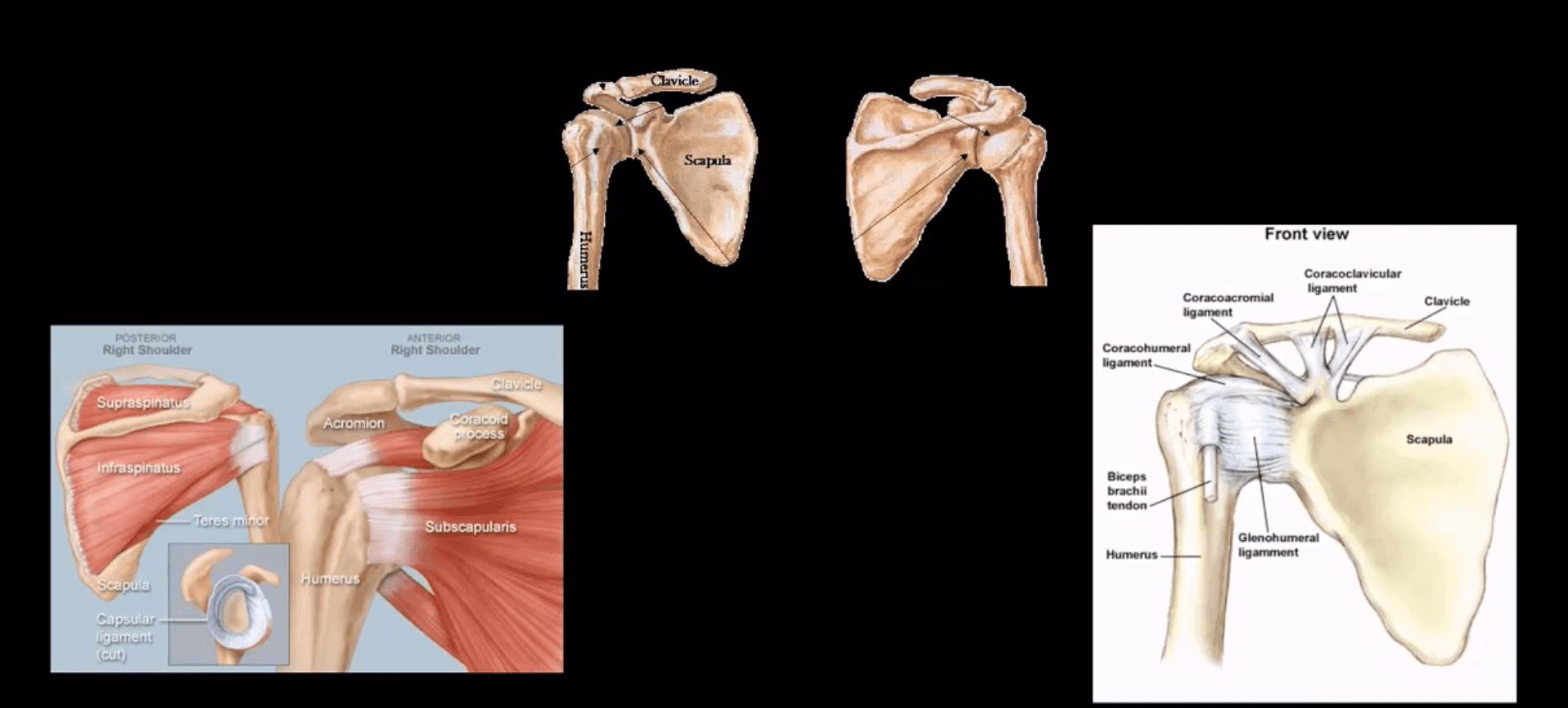
Anatomy: Shoulder stability is sacrificed for mobility, and overall GHJD is the m/c among large joints in the body
Protective falls (e.g., FOOSH) and MVA are m/c causes. GHJ is most vulnerable in abduction, extension and external rotation. Anatomical factors: shallow glenoid, laxed ant-inferior capsule and GH ligaments. GHJD will induce severe tearing of major GHJ restraints. Associated osseous and labral injuries are common and may lead to chronic instability, DJD,�and functional changes
3-types: Anterior GHJD (95%)
Posterior GHJD (4%) especially associated with epileptic seizures, electrocution and can occur b/l
Inferior GHJD aka Laxatio Erecta (<1%) associated with severe trauma
Clinically: AGHJD presents with severe pain, the arm is externally rotated and adducted, severe limitation of movement. GHJD may persist as chronic dislocation.
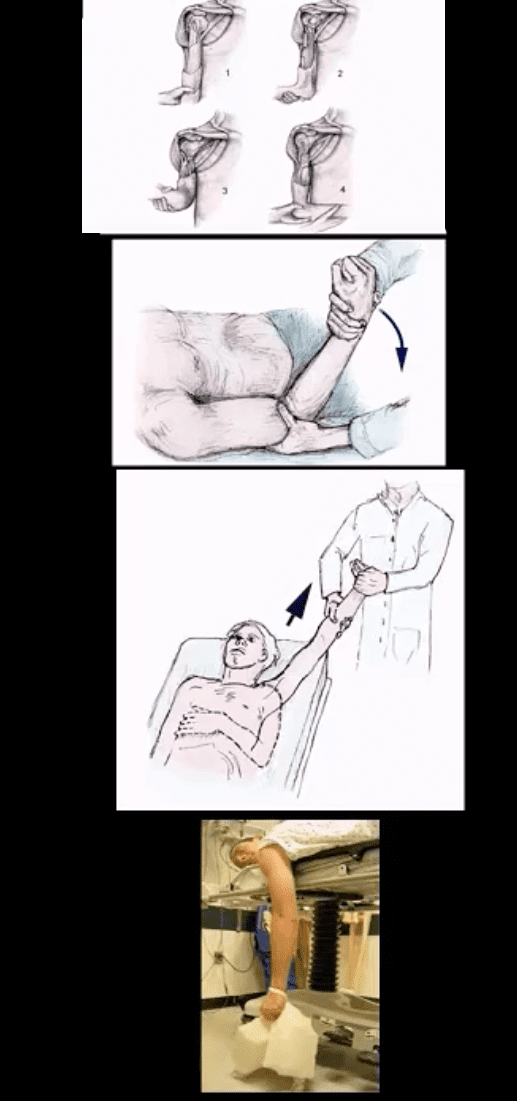
Management: prompt reduction in ED under anesthesia or heavy sedation with Kocher technique top image (not used), External rotation method (middle) or Milch technique (can be used w/o anesthesia) and a few other methods. Delay in reduction correlates with greater risk of immediate and long-term�complications
Diagnostic Imaging Approach
Shoulder series x-radiography is sufficient. Additional Imaging with CT scanning and MRI may be helpful to Dx osseous, cartilage, labral/ligaments pathology
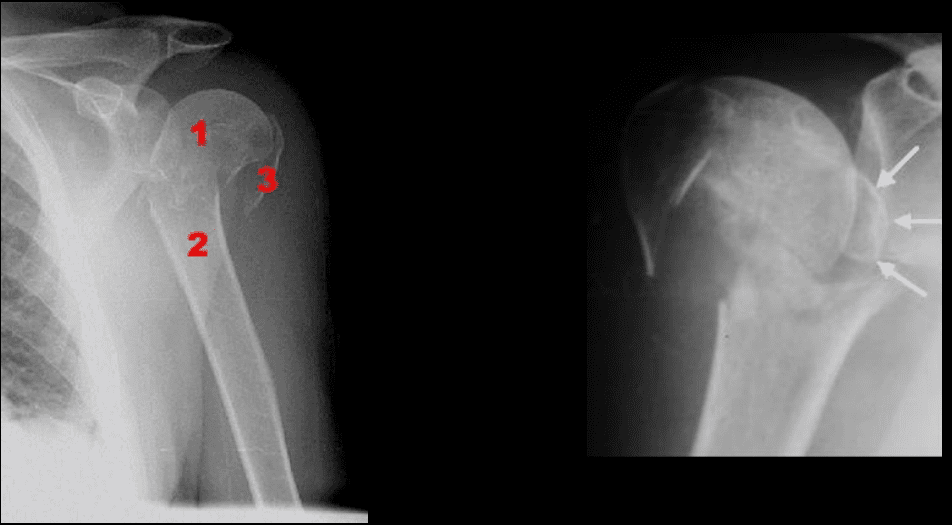
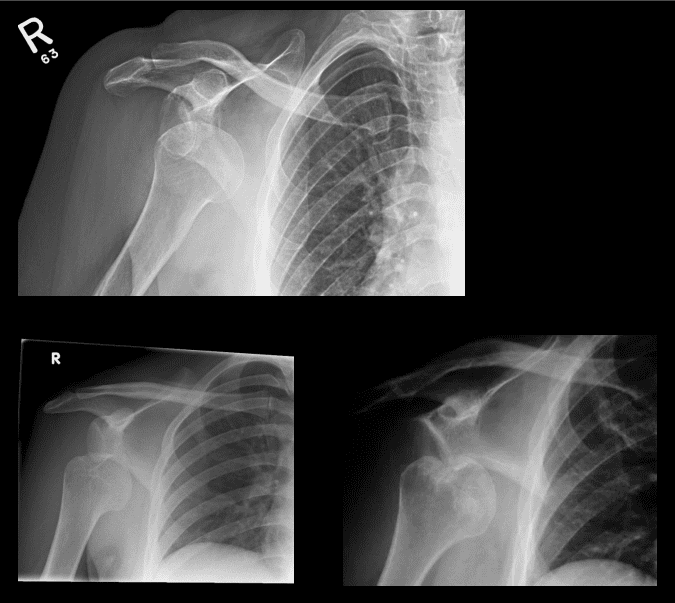
Anterior GHJD (95%). Subcoracoid position(top right) of the humerus is the m/c
Anterior GHJD may also occur as subglenoid(bottom left)and infrequently as subclavicular
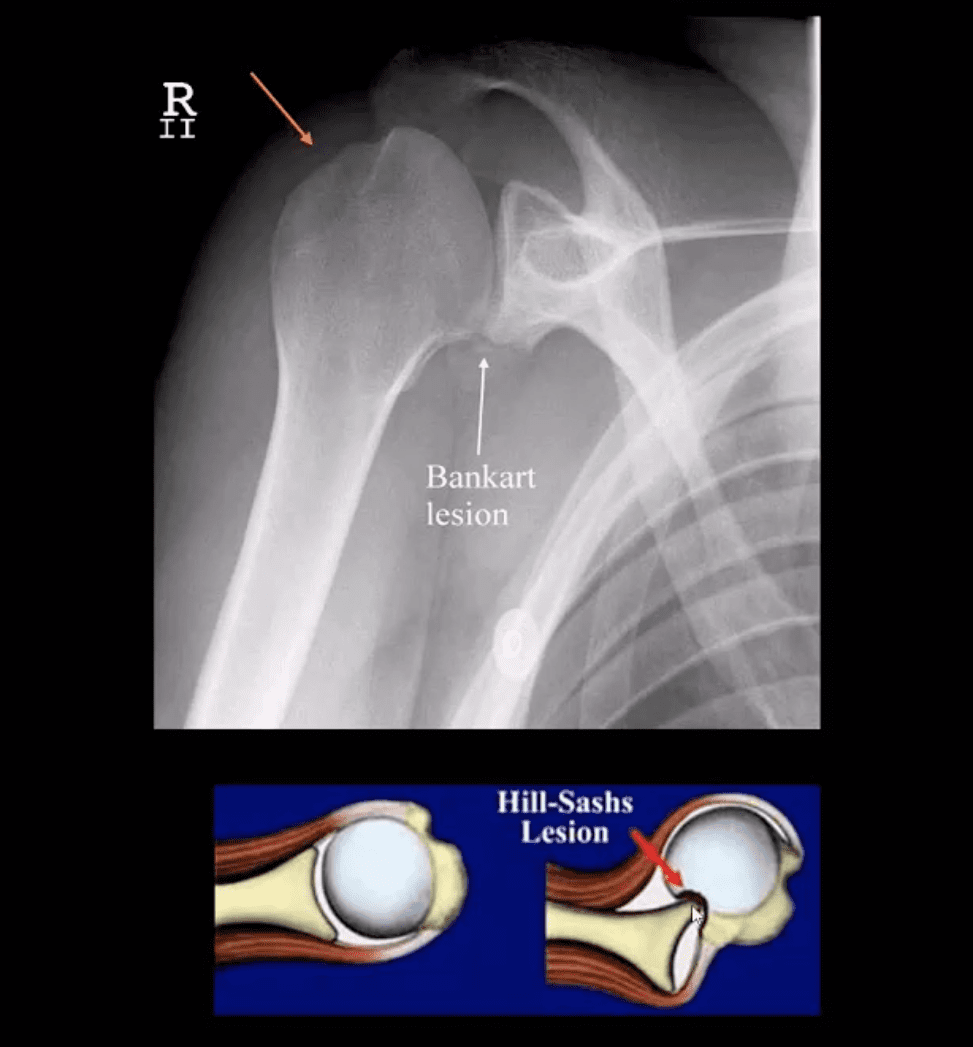
Key to radiographic search is to evaluate associated Bankart and Hill-Sachs injuries
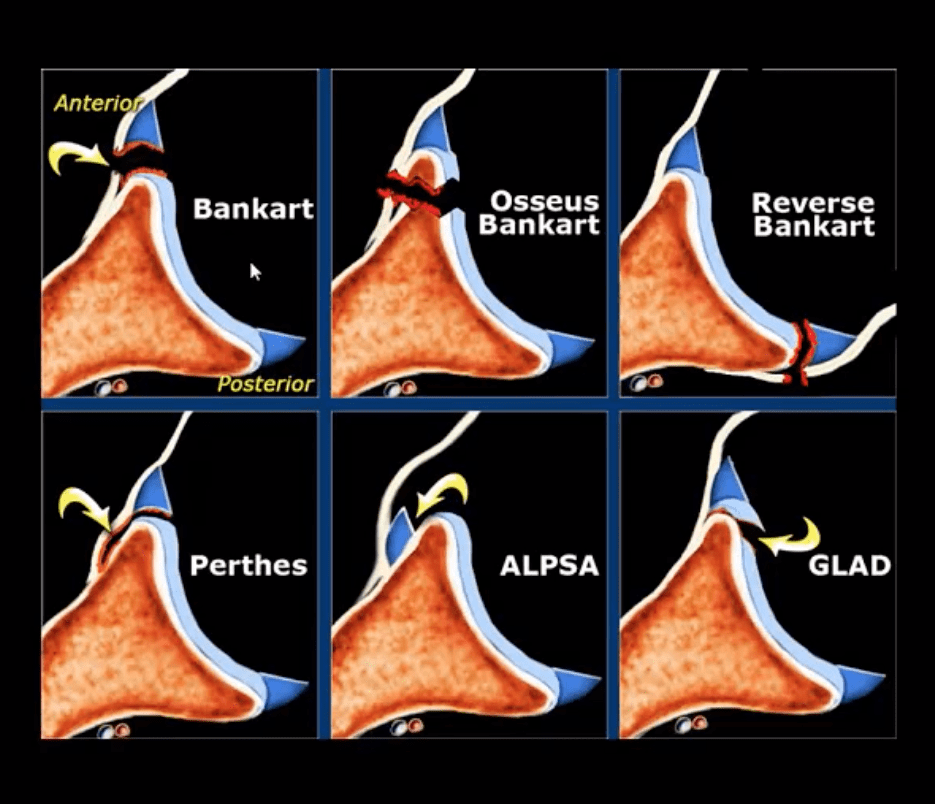
Bankart Lesion
Occurs during anterior GHJD d/t impaction of the head into anterior-inferior glenoid. Variations exist (see next slide). BonyBankart can be seen on x-rays. So-called soft tissue Bankart requires MRI. Cartilage (soft)Bankart is the m/c.
Hill-Sachs aka Hatchet deformity (arrow postreduction)occurs during the same mechanism as Bankart, i.e., compression and impaction of posterolateral aspect of the head against the glenoid producing wedge-shape Fx. Hill-Sachs lesion may predispose to recurrent/chronic GHJD.
Bankart lesion may heal, but operative suture anchors are needed sometimes
CT arthrogram and MRI may be helpful
Types of Bankart Lesion
Note different types of Bankart lesion. Onlyosseous Bankart can be seen radiographically. Soft tissue Bankart requires MRI with and without intra-articular gadolinium(arthrogram).
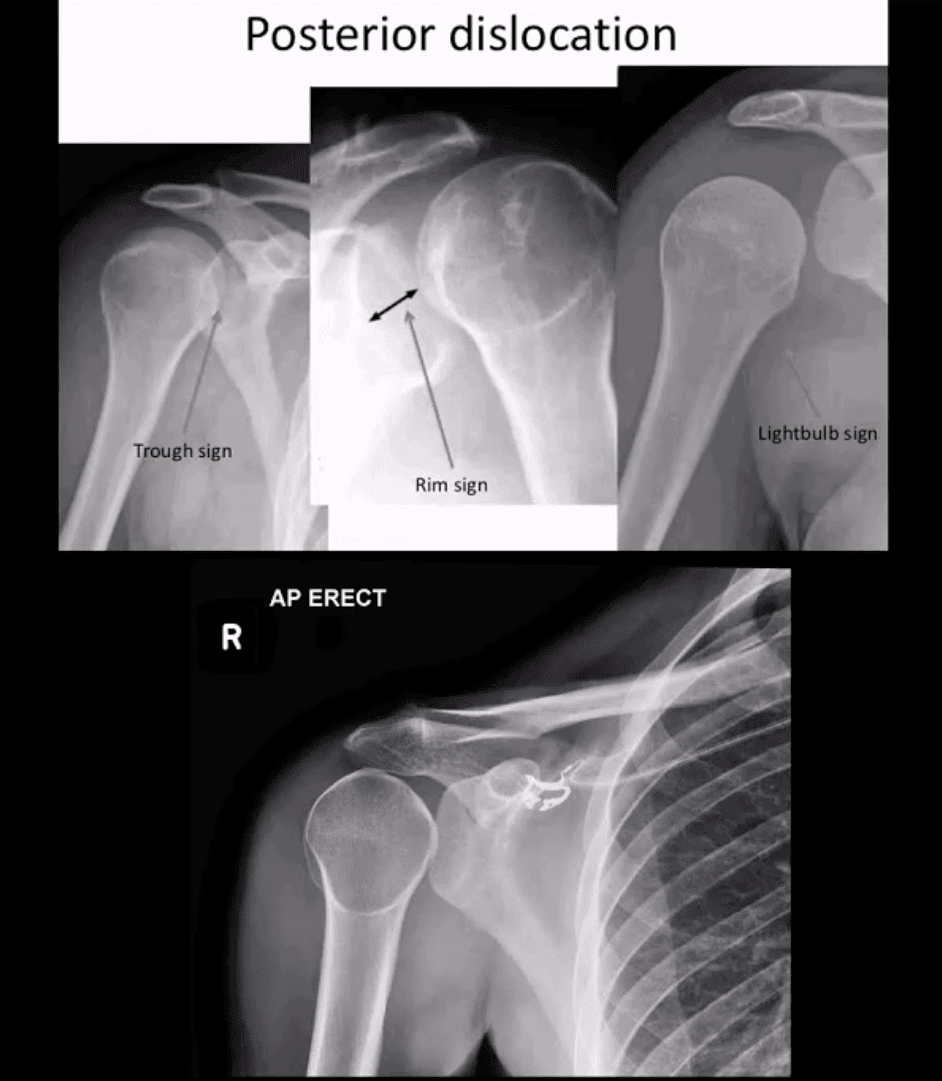
Posterior Dislocation
Note: posterior GHJD with its characteristic signs:
Trough sign aka reverse Hill-Sachs. Occurs d/t anterolateral head impaction Fx
Rim sign: only occurs in the PGHJD d/t posterior position of the head and anterior glenoid-to humeral head distance 6-mm or greater
Light-bulb sign: d/t acute internal rotation of the humerus (head)
Inferior GHJD
Inferior GHJD aka Laxatio Erecta
Severe hyperabduction and inferior displacement of the humerus. Greater chances of severe neurovascular injury and acromial Fx
The dislocated arm is hyperabducted and fixed with the elbow flexed and the arm above the head
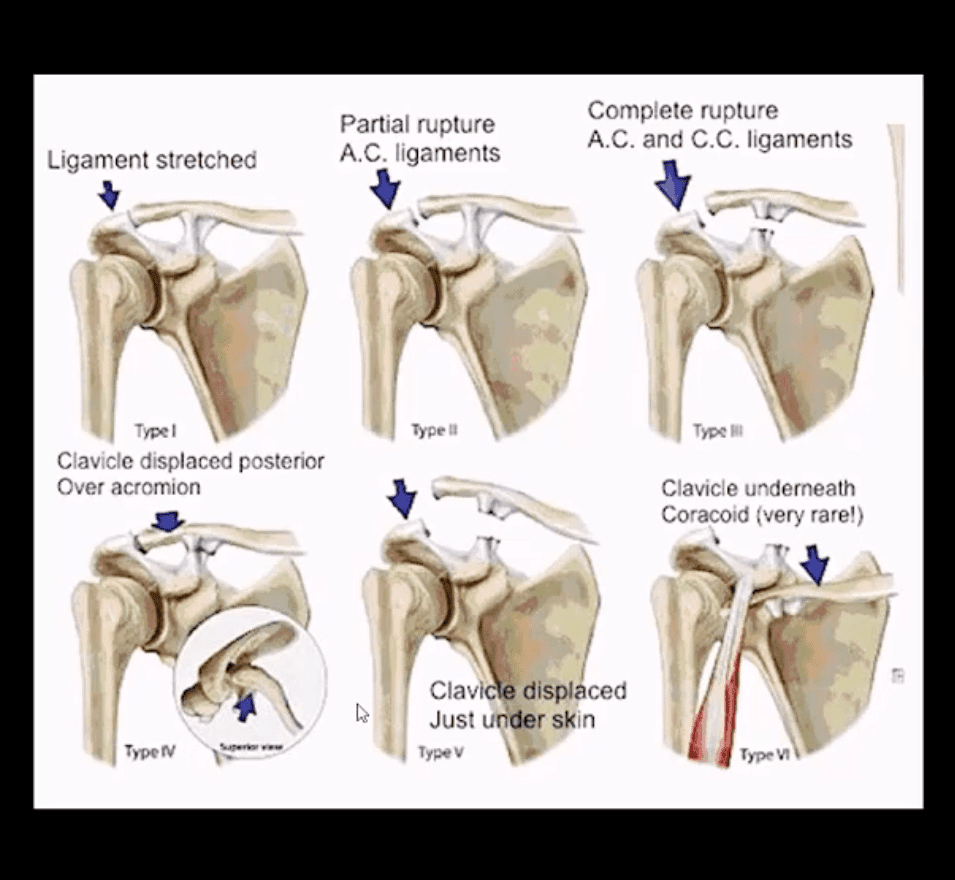
ACJ Dislocation (ACJD)
ACJD: common injury, 9% of shoulder girdle injuries esp. in male athletes by a direct blow
Rockwood classification (left) evaluates tearing of AC and CC ligaments and regional muscles
Type1, 2, 3 among the m/c
Type 1: sprain of ACL w/o tearing
Type 2: tear of ACL and sprain of CCL
Type 3: tear of AC & CCL. The clavicle is elevated above the acromion. If <2-cm good results with conservative Rx.
Imaging: x-radiography with b/l ACJ views with and w/o weights to compare both ACJs. In complex cases CT scanning esp. if Fx is considered
Management: Type 3 (>2-cm) & Types 4-6Operative
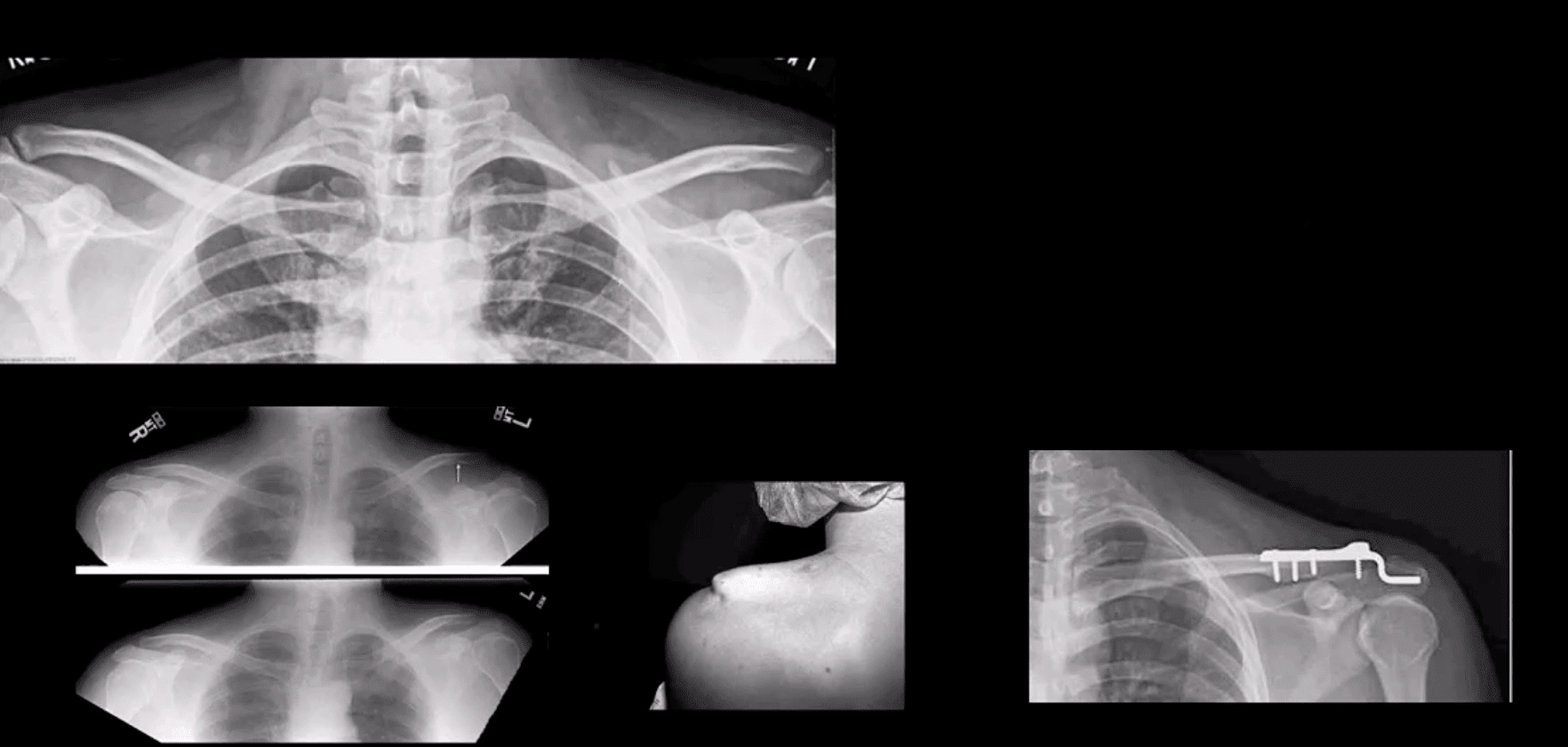
Type 3 ACJ Separation
Type 3 ACJ separation (top left)
More significant ACJD (bottom images) with clinical sign of acromion under the skin and resultant ORIF
Rotator Cuff Muscles (RCM) Pathology
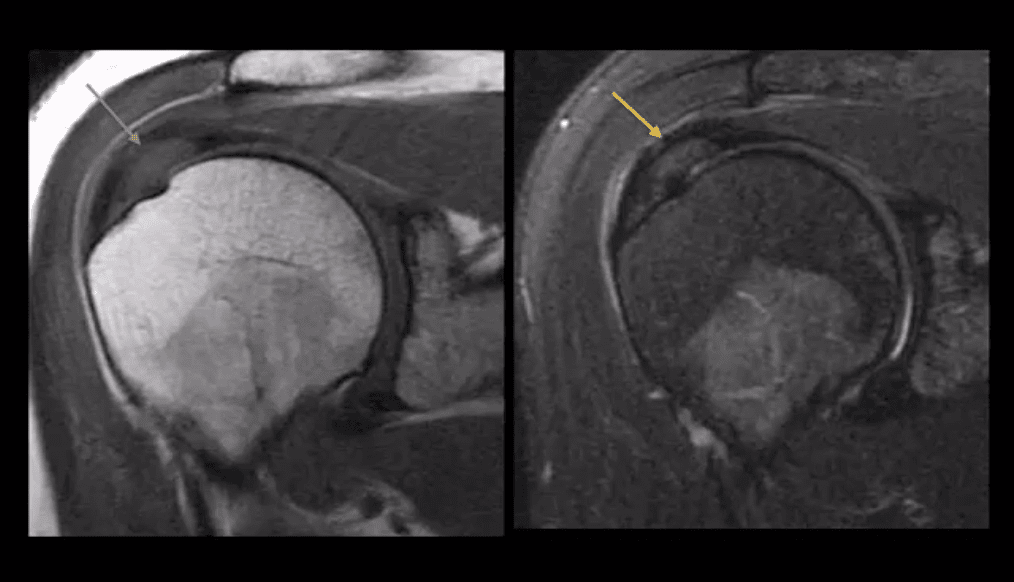
RCM tendinopathy: collagenous degeneration of RCM particularly Supraspinatus M. tendon(SSMT) d/t overuse/degeneration-micro tearing with collagenous replacement. Impingement syndrome is a 2nd extrinsic cause. Presented clinically as pain and limited ROM
Imaging Dx: MSK US can be as accurate as MRI and better in some cases d/t dynamic evaluation v. cost effective
Key MRI clue is thickened inhomogeneous SSMTwith increased signal on all pulse sequences d/t fatty degeneration and inflammation (left images: T1 & T2 FS)
MSKUS findings: thickening of the SSMTsubstance with a change�in normal echogenicity.MSKUS is good to DDx with SSMT tears. US advantages are that it allows dynamic evaluation of painful structures
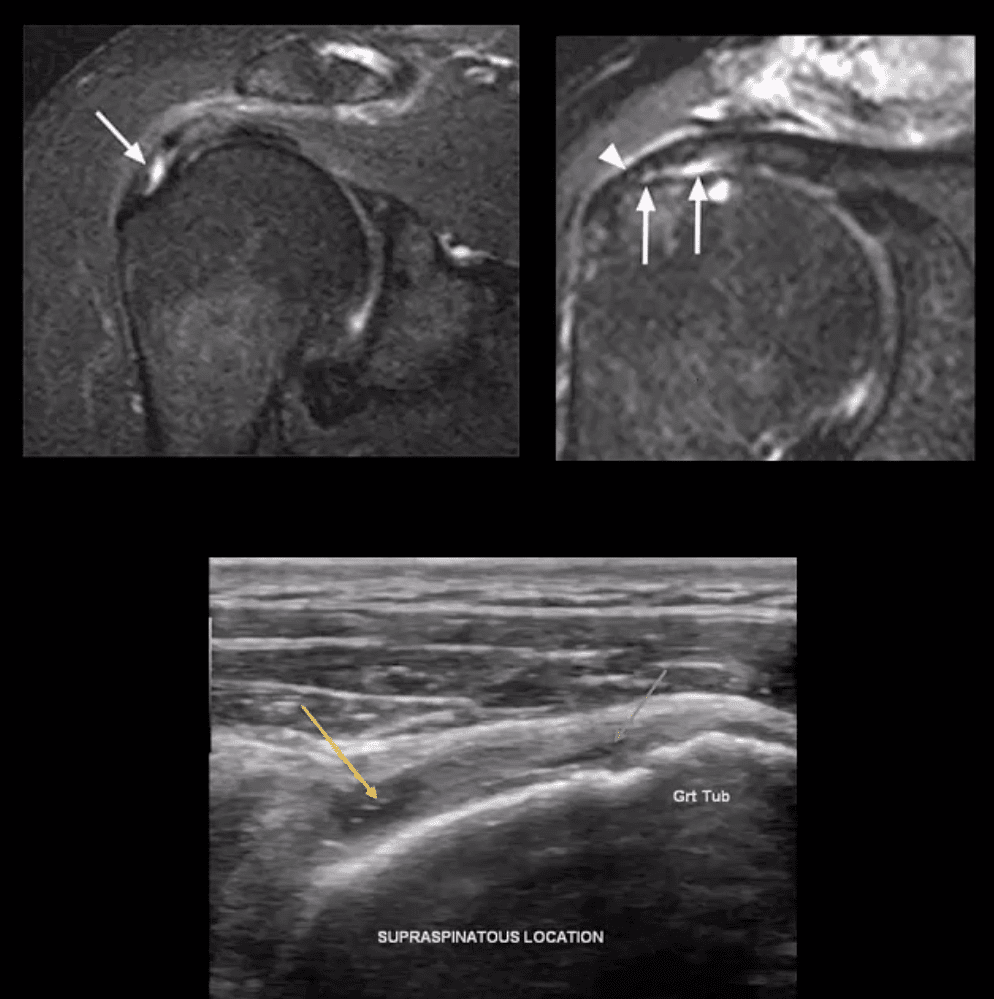
Partial tear of SSMT: partial (incomplete) tear ofSSMT may occur at the bursal and articular surface or interstitial, i.e., intra-substance/noncommunicating. Etiology: sub-acromial impingement, acute strain, and chronic microtrauma tendinosis
Clinically: pain on abd and flexion, impingement tests, Hawkins-Kennedy tests, etc. Pearls: partial tears can be more painful than complete tears
Imaging Dx: MSKUS is as good as MRI (N.B.some studies indicated MSKUS is more superior to MRI). Key MRI findings: gap/incomplete tear of SSMT filled with joint fluid +/- granulation tissue
MSKUS: decreased echogenicity of SSMT, thinning and partial tearing filled with fluid(anechoic areas arrows). Lost convexity of tendon bursal or articular interface.
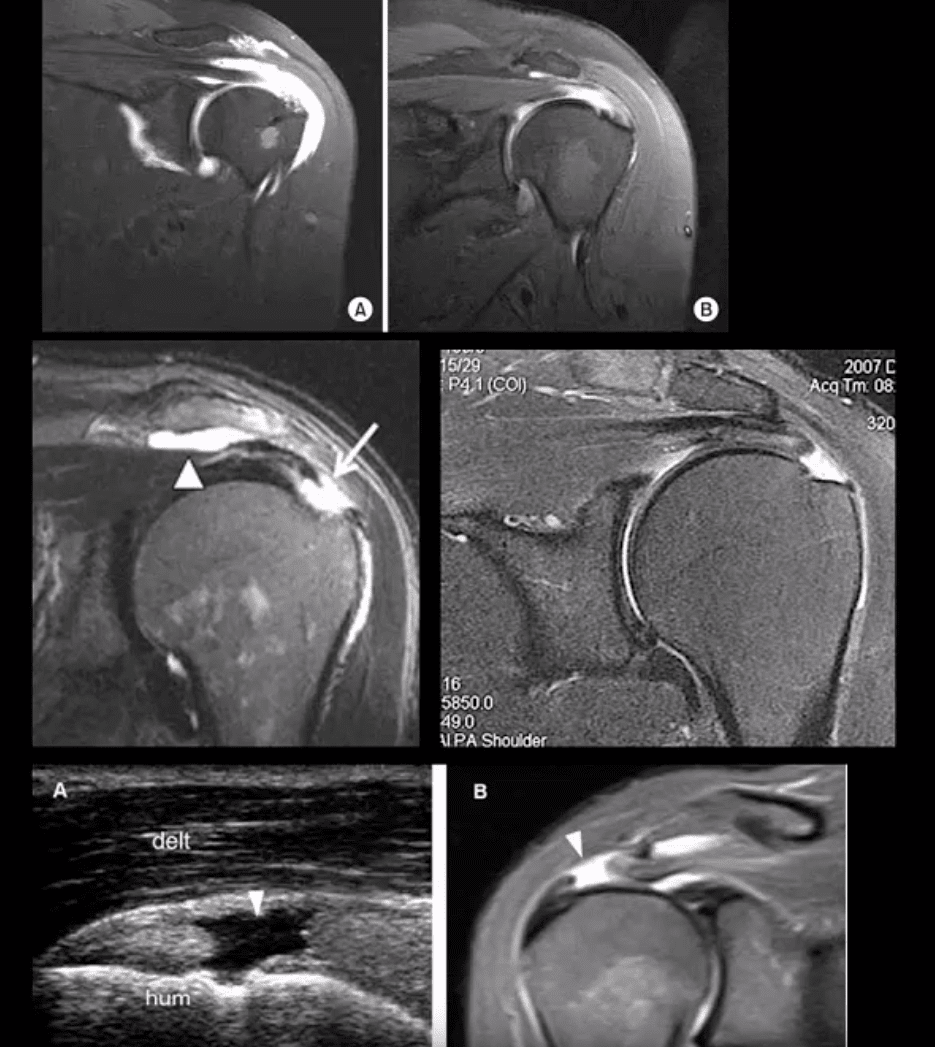
Full Thickness SSMT (rot cuff) tear: degeneration/tearing of rot cuff. 2nd to impingement by Hooked acromion, overhead overuse or acute trauma. 7-25% of shoulder pain in the general population. Clinically: pain on impingement tests.
Imaging Dx: MSKUS is as good as MRI.Limitations: poor Dx of labral pathology. Key USDx: focal tendon interruption, an anechoic gap (fluid filled), hypoechoic tendon, tendon retraction, uncovered cartilage sign (bottom left, A: US B: MRI)
MRI: key Dx: insertional tear extending through entire SSMT crescent, retraction with fatty degeneration of SSMT and the muscle. If retraction is at 12 o�clock or greater (top images), it may not be anchored operatively
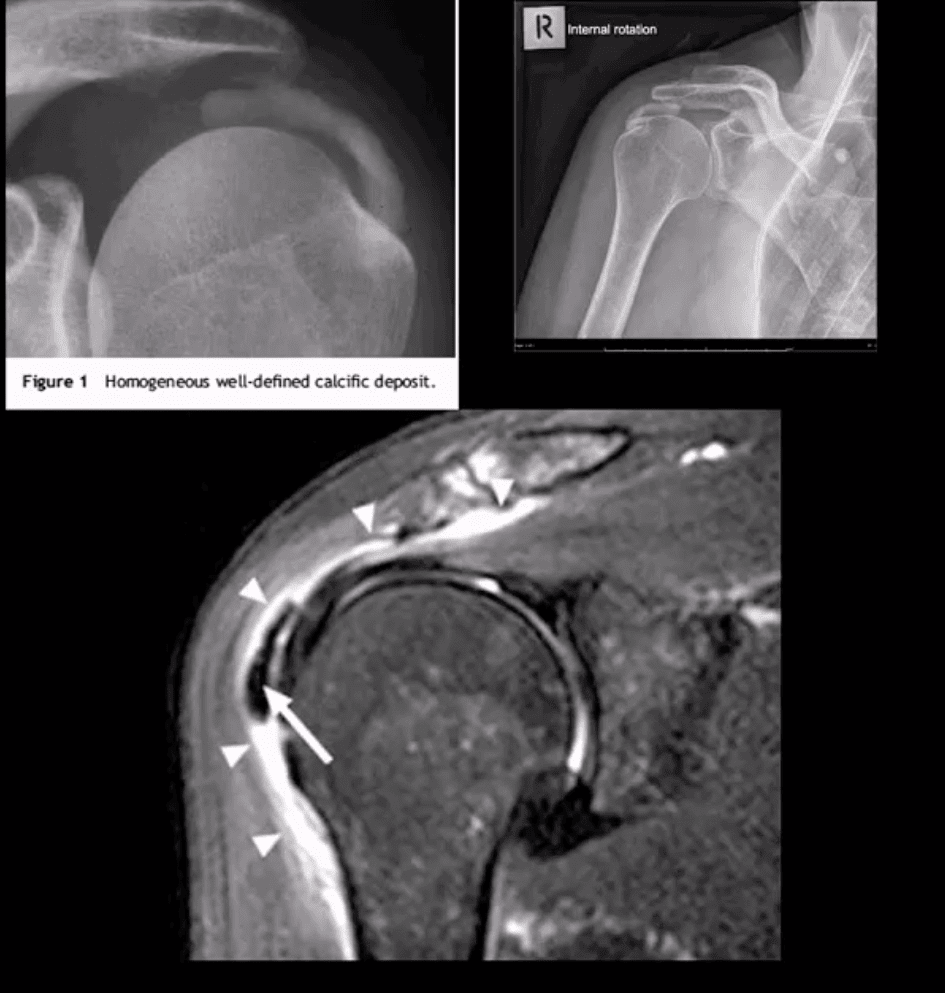
Rotator Cuff (RTC) Calcific Tendinitis: usually d/t calcium HADD crystals. Middle-aged women are most affected. Ranges from asymptomatic imaging finding to severe destructive arthropathy or Milwaukee shoulder(infrequent)
HADD has 3-pathological phases: formation resting-resorption.Mild-to-moderate pain esp. in resting phase.
Imaging: x-radiography: homogenous ovoid mineralization within RTCMT, m/c in SSMT. MRI: ovoid/globular decreased signal on all pulse sequences often with surrounding edema (bottom left)
Rx: self-resolution occurs. Advanced cases: operative aspiration etc.
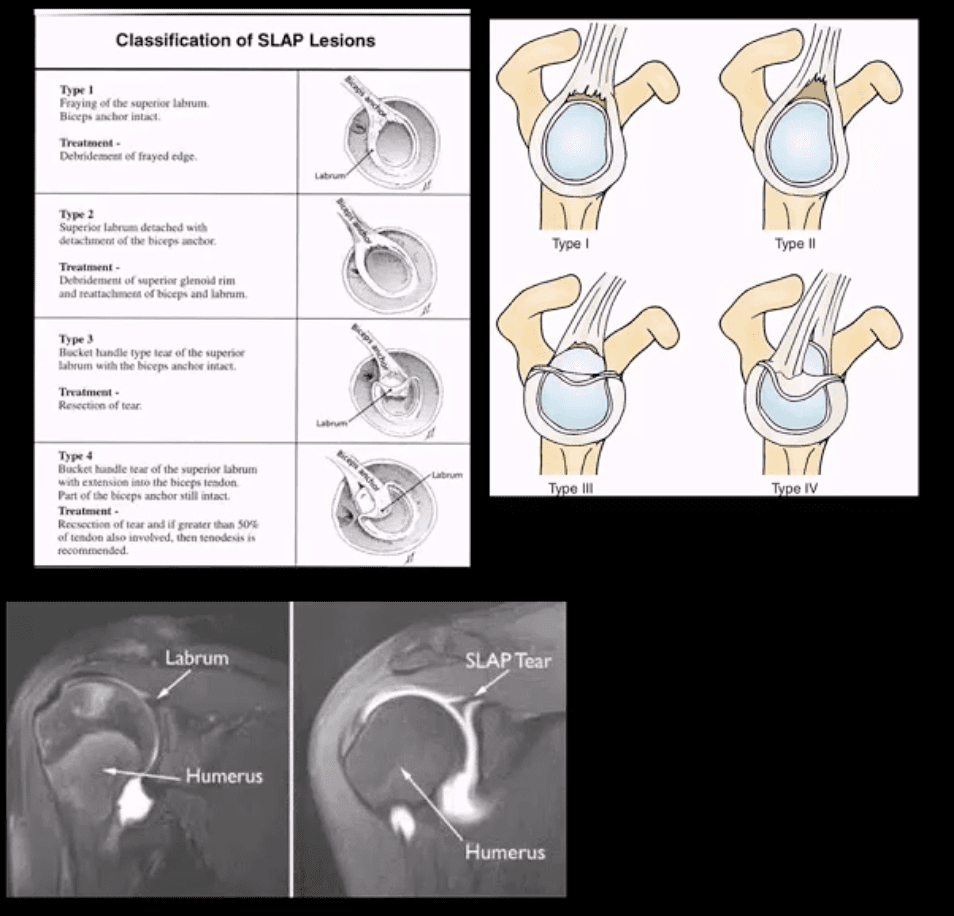
Superior Labrum Anterior to Posterior (SLAP) Lesions/Tears
SLAP tears: FOOSH and throwing sports or chronic shoulder instability aka Multidirectional shoulder instability (in 20%). Type 1-9 exist but the M/C areType 1-4
In all 4-types superior labrum is affected with or w/oLHBMT anchor tear (see pictures). Clinically: pain, limitation of AROM with active compression tests, typically non-specific findings mimicking RTCpathology
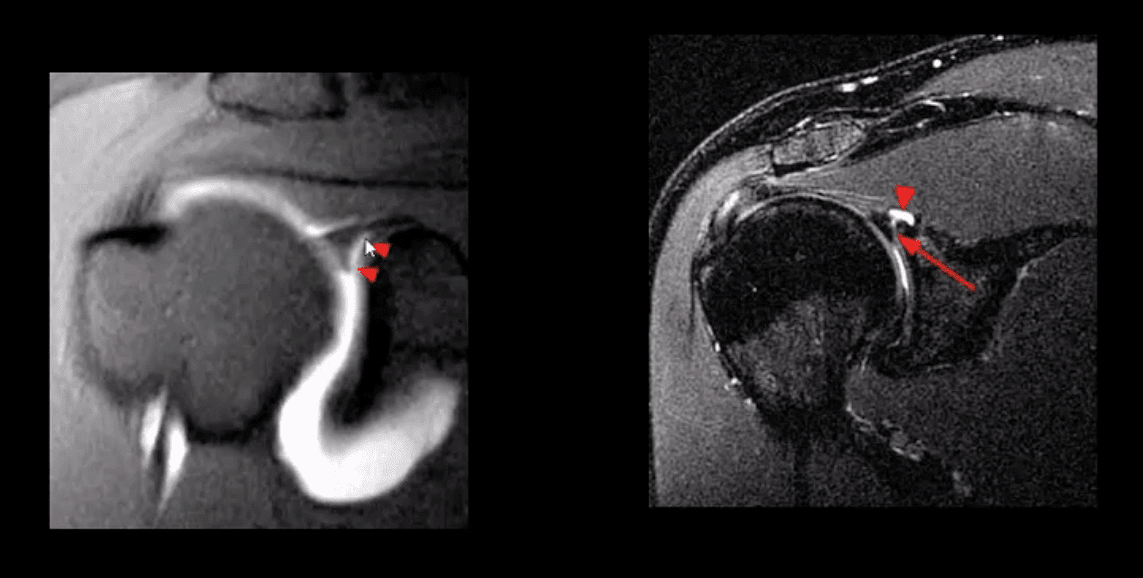
Imaging is crucial: best imaging is MRI arthrography. Key signs: hyperintense linear fluid signal within superior labrum +/- extending along the LHBT on fat-suppressed fluid sensitive imaging and FS T1 arthrogram. Best observed on coronal slices.
Rx: small tears may heal, but unstable tears require operative care.
Key DDx: anatomical variants like Buford complex andSub-labral foramen
SLAP tear with a paralabral cyst (bottom right)
Normal variant DDx: sub labral foramen(bottom left) note: MR arthrography with contrast undercutting the labrum but w/o extending posteriorly to the LHBT
Shoulder Arthritis
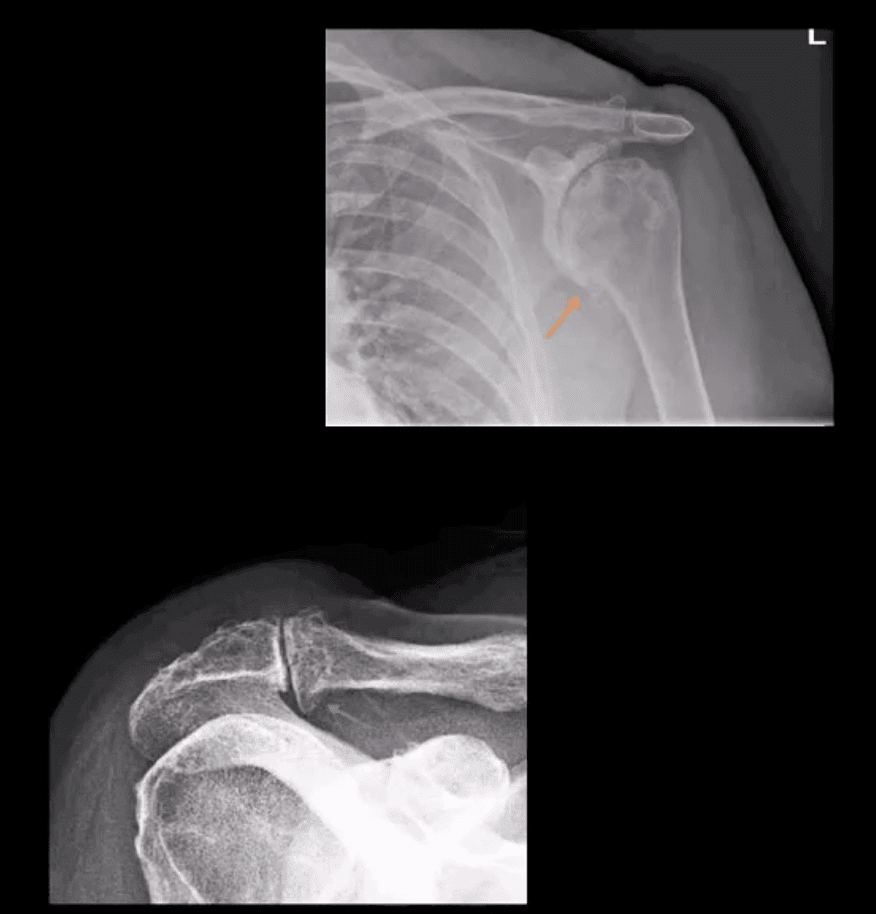
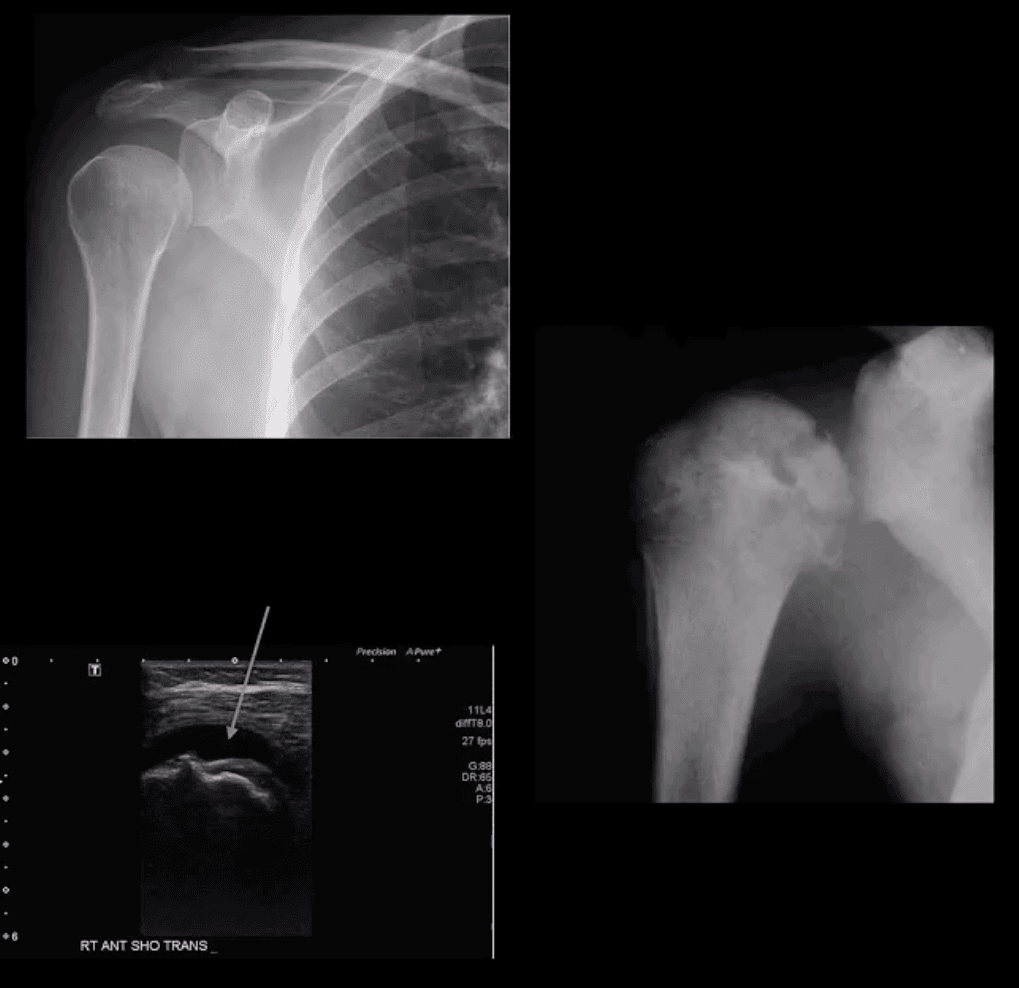
GHJ DJD: usually associated with a 2nd cause: trauma, instability, AVN, CPPD, etc. Presented with pain, crepitus and decreased ROM/function. Associated RTC disease may be present. Imaging; x-radiography is sufficient and provides grading/care planning.Major findings: joint narrowing, osteophytosis esp. at the inferior-medial head (orange arrow), subchondral sclerosis/cysts. Often noted superior head migration d/t RTC disease.
ACJ OA: common and typically primary with aging. Presents with ACJ loss and osteophytes. Osteophytes along the undersurface of the ACJ �keel osteophytes�(blue arrow) may lead to RTC muscle tear. Regional bursitis is other clinical feature of ACJ arthrosis.
Management: usually conservative depending on clinical signs/symptoms
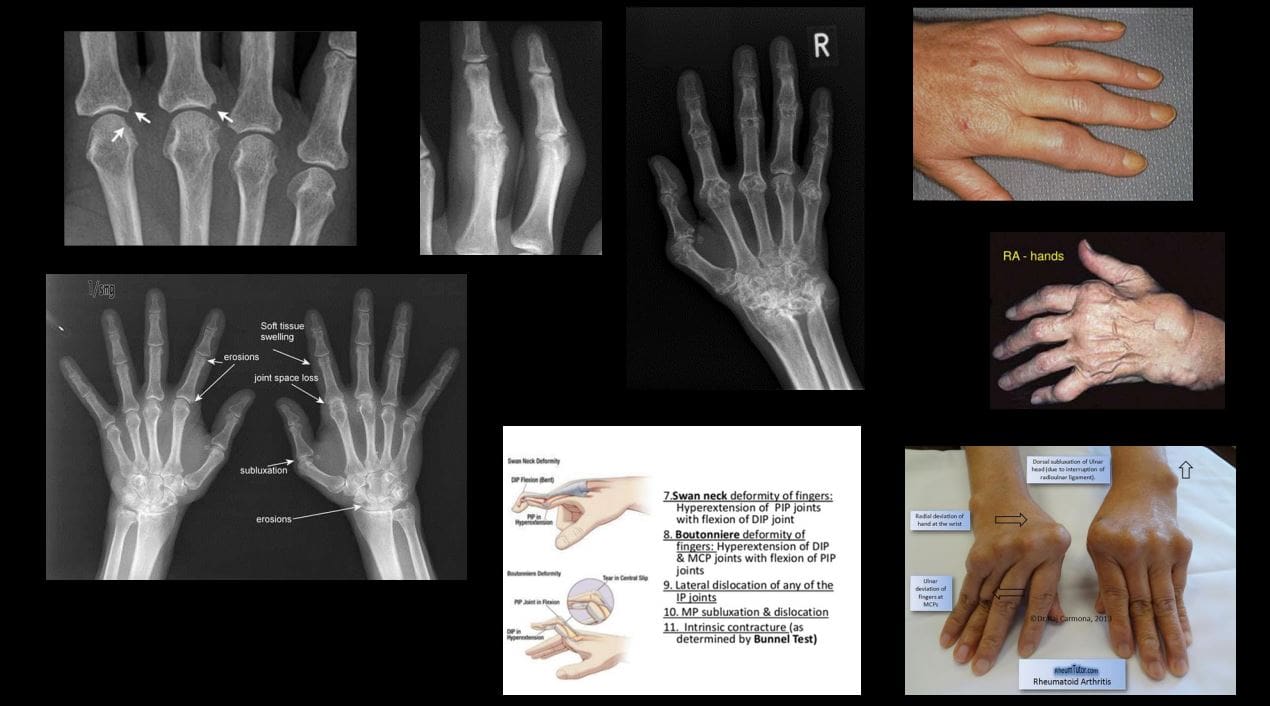
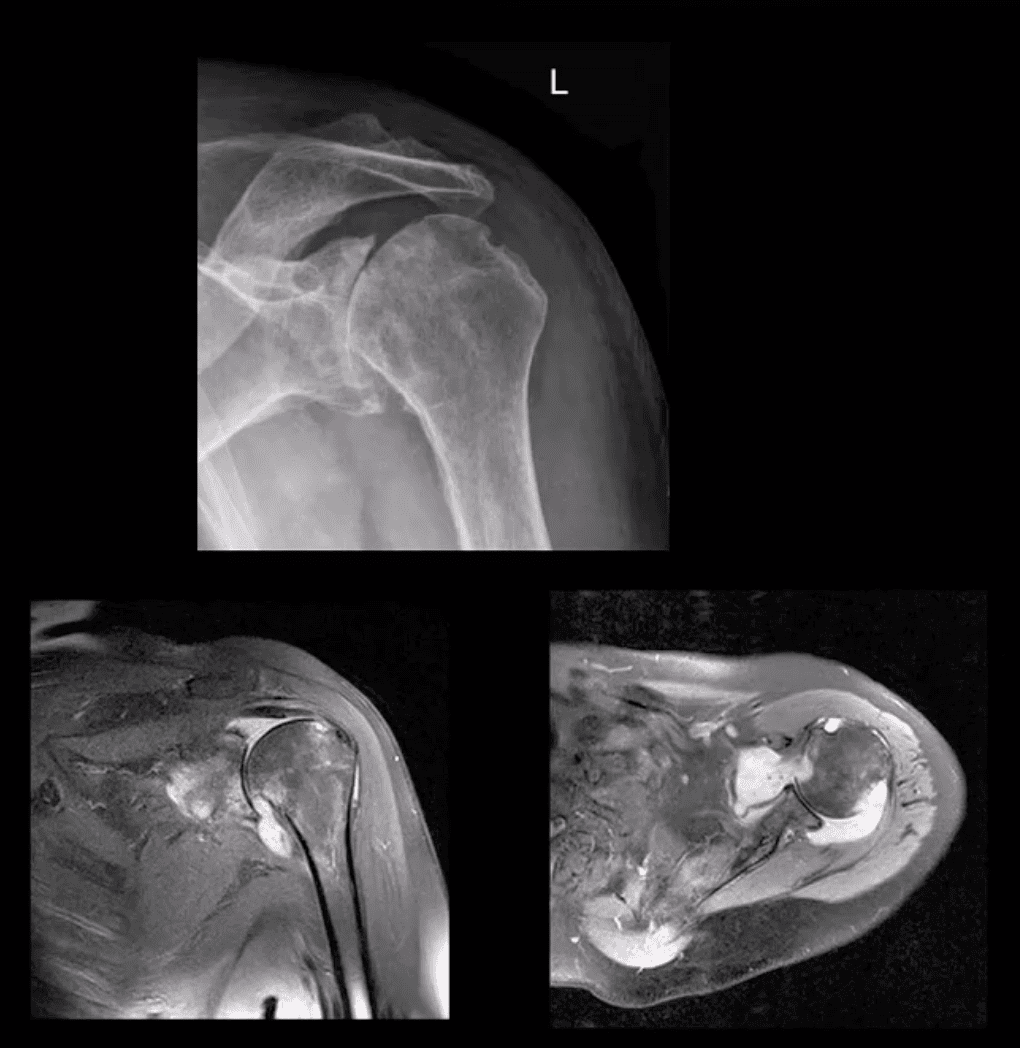
Rheumatoid Arthritis GHJ: RA is a multisystem inflammatory disease affecting multiple joints lined by the synovium. GHJ RA is common (m/c large joints in RA knees/shoulders). Clinically: pain, limited ROM and instability, muscle weakness/wasting. Hands, feet,�and wrists are m/c affected. Imaging: x-radiography reveals periarticular erosions, uniform joint space loss, juxta-articular osteoporosis, subluxations,�and soft tissue swelling. MRI can help detect�commonly associated RTC tearing and instability. Early changes can be detected by MSKUS esp. with power Doppler use indicating hyperemia/inflammation.
Note: L shoulder x-ray revealing cartilage destruction and symmetrical joint loss, multiple erosions, and likely loss of RTCM support with superior head migration, ST effusion present.
Note: PDFS coronal and axial MRI slices of GHJ RA indicating marked inflammatory joint effusion, bone erosion/edema, synovial pannus formation and likely tear in RTC m. Management: Rheumatological referral and pharmacotherapy with DMARD. Operative care asRTCM repair. 10% of patients are disabled d/t RA
Neuropathic Osteoarthropathy aka Charcot’s shoulder: d/t neurovascular and neural periarticular damage. Multiple causes exist.M/c develops in diabetics in midfoot. Shoulder Charcot is m/c in Syringomyelia (25%), trauma paralysis, MS, etc. Dx: clinical(50% pain/swelling 50% painless destruction). Imaging is crucial. X-radiography is sufficient in well-established cases, but early Dx is challenging. MRI may help with early Dx and delayed complications. Rad Dx: Shoulder Charcot is m/c presented as atrophic type destructive arthropathy with humeral head appearing as if surgically amputated along with intra-articular debris, density, distention, dislocation, and other key features
Septic Shoulder: shoulder is the 3rd m/c followingknee>hips. Patients at risk: diabetics, RA pts, immunocompromised, I.V. drug users, indwelling catheters, etc. Routes: hematogenous (m/c), direct inoculation (iatrogenic, trauma etc.) adjacent spread(e.g. OM). Staph. Aureus (>50%) m/c.
Clinically: joint pain and dec. ROM, fever 60% only, toxemia, inc. ESR/CRP. Dx: imaging and joint aspiration/culture. RadDx: early x-rays often unremarkable except ST effusion/fat planes obscuration, joint widening. Later7-12 days patchy osteopenia, moth-eaten/permeating bone resorption, articular destruction, joint narrowing. May progress to severe joint destruction and ankyloses. Early Dx & I.V. antibiotics are crucial even before culture. Operative irrigation and joint drainage in some cases. Complications are possible esp. if Rx is delayed. MSKUS with needle aspiration may help. Note: (top image) non-traumatic joint widening with inferolateral head displacement d/t septic A dx: by needle aspiration Staph. Aures.
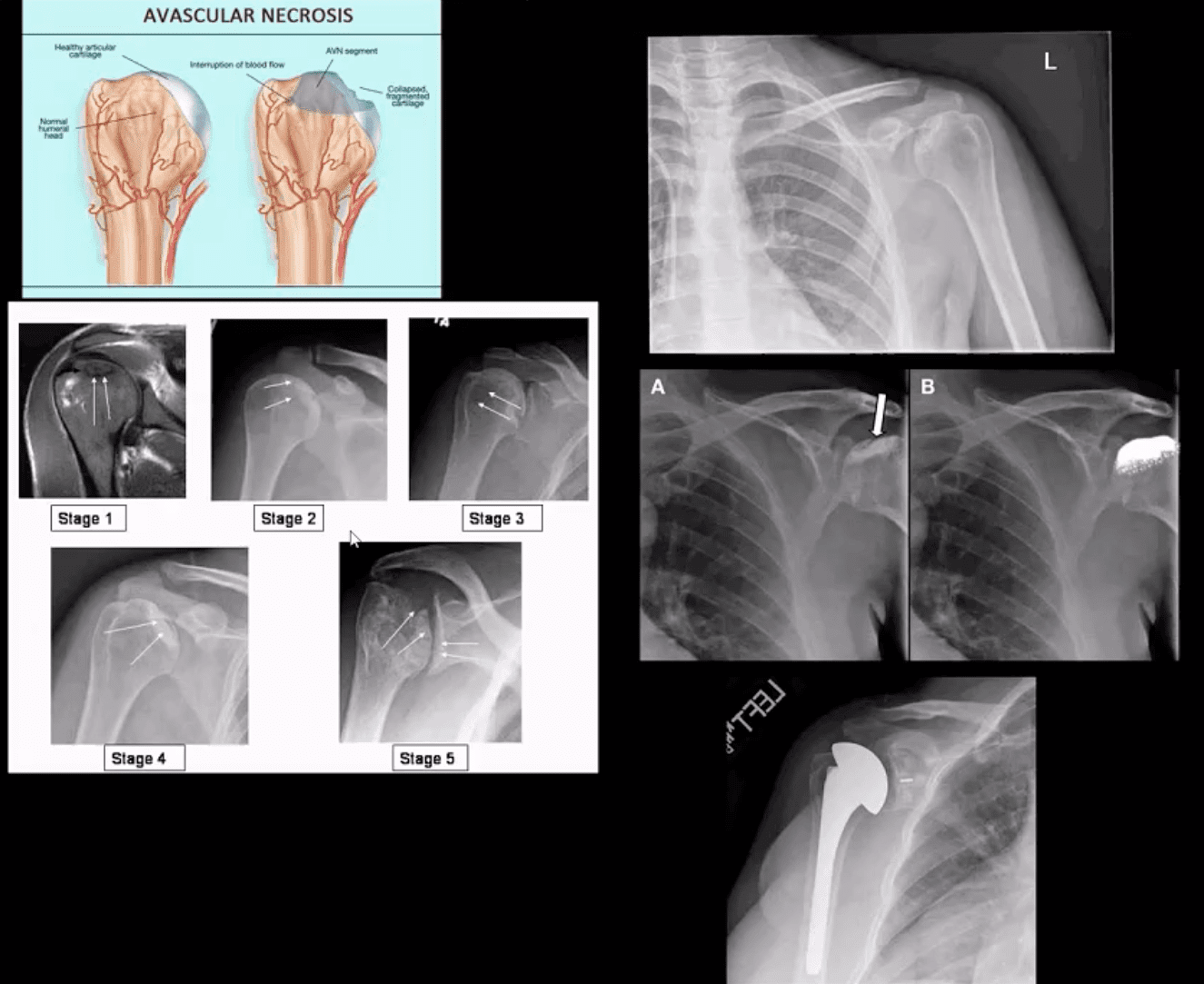
Ischemic Osteonecrosis
Ischemic Osteonecrosis of the humeral head may occur d/t trauma (Neer four-part Fx), Steroids, Lupus, Sickle cell, Alcoholism, Diabetes,�and many other conditions. Imaging is crucial: MRI detects earliest changes as intraosseous edema. X-ray features are late, presented as a collapse of subchondral bone with sclerosis �snow cap� sign, fragmentation, and progressive severe DJD
Management: orthopedic referral, core decompression in early cases, hemiarthroplasty in moderate and total arthroplasty in severe cases.
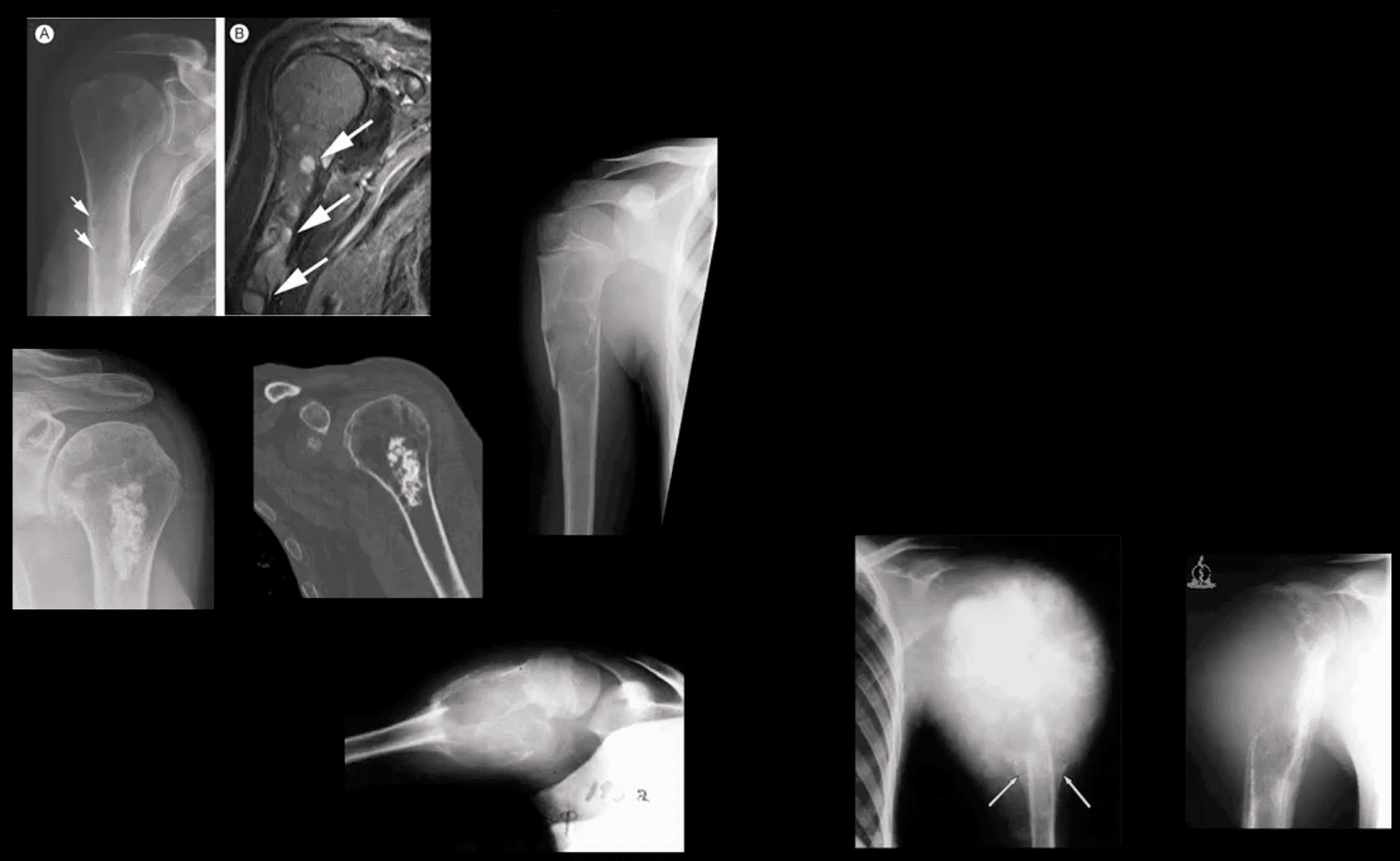
Shoulder Neoplasms
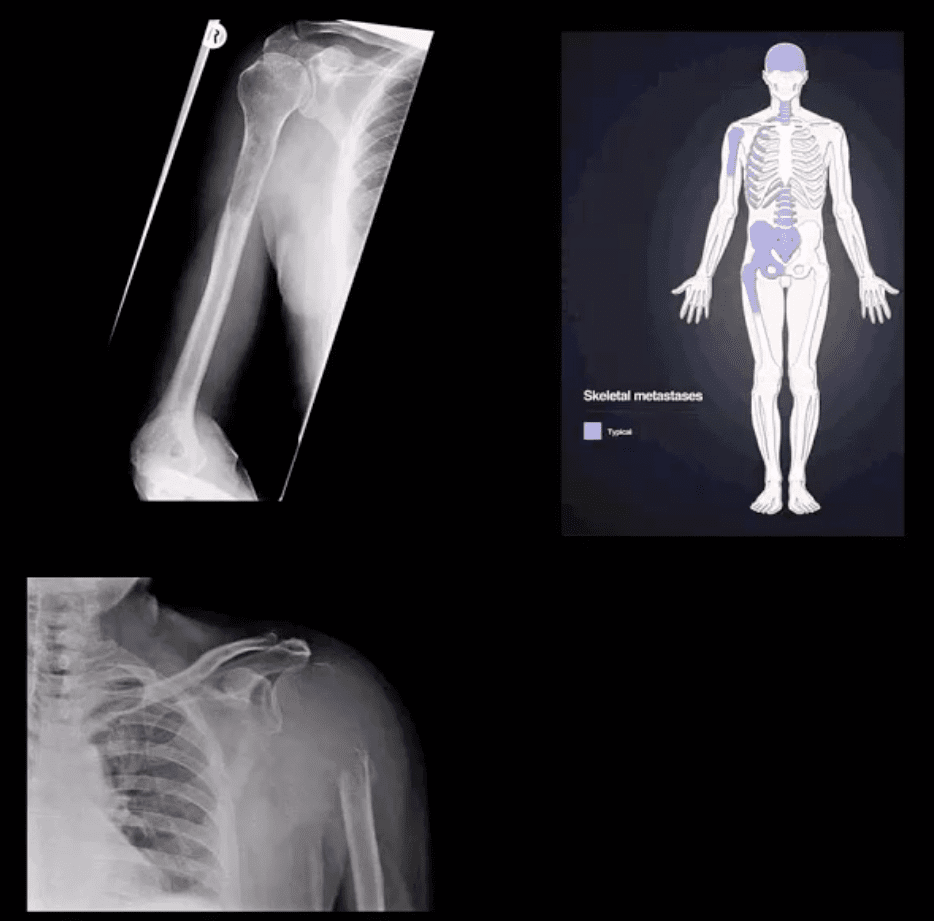
In adults >40, bone Mets d/t lung, breast, renal cell, thyroid CA & prostate are the m/c causes. Clinically: may mimic pain resemblingRTC/joint changes. Should be evaluated carefully. Key to Dx: Hx, PE and Imaging esp.in pts with known primary
Imaging: 1st step x-rays, MRI can help, Tc99bone scintigraphy helps to detect regional and distant disease. X-ray features: destructive lytic changes typically in prox humerus(red marrow) with or w/o path Fx. DDx: Mets, MM, lymphoma
Clinically: night pain, pain at rest, etc. Lab tests: unrewarding, in severe cases hypercalcemia may be noted.
Primary Malignant bone neoplasms (shoulder) Adults: M. Myeloma or Solitary plasmacytoma, Chondrosarcoma may transform from an enchondroma and some others. In children/teenagers: OSA vs. Ewing�s
Primary benign bone neoplasms (shoulder). Adults: Enchondroma (patients in their 20-30s)GCT. In children: Simple bone cyst (Unicameral Bone cyst), Osteochondroma, Aneurysmal Bone Cyst, Chondroblastoma (rare)
Imaging: 1st step x-radiography
MRI is essential to Dx. Especially in cases of primary malignant neoplasms Evaluate extent, soft tissue invasion, preoperative planning, staging, etc.
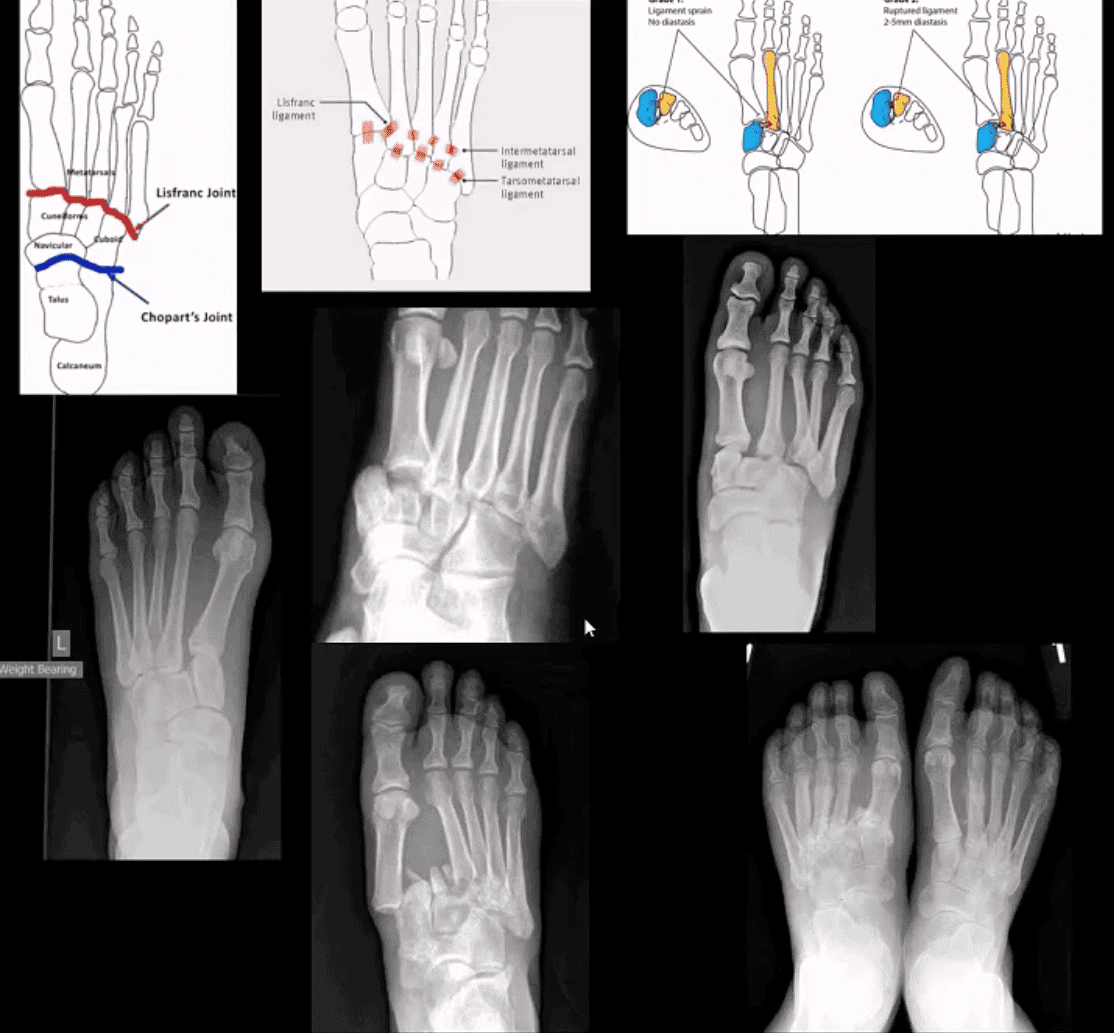
M/C dislocation of the foot at tarsal-metatarsal articulation (Lisfranc joint). Direct impact or landing and plantar or dorsal flexing the foot. Lisfranc ligament holding 2nd MT base and 1st Cu is torn. Manifests with or w/o fracture-avulsion.
Imaging: 1st step: foot radiography in most cases sufficient to Dx. MSK US may help: show disrupted Cu1-Cu2. Ligament and widened space > 2.5mm. MRI may help but not essential. Weight-bearing view aids Dx.
2-types: homolateral (1st MTP joint in contact) and divergent (2-5 MT displaced laterally and 1st MT medially)
Management: operative fixation is crucial
N.B. Atraumatic Lisfranc dislocation is a frequent complication of a diabetic Charcot foot
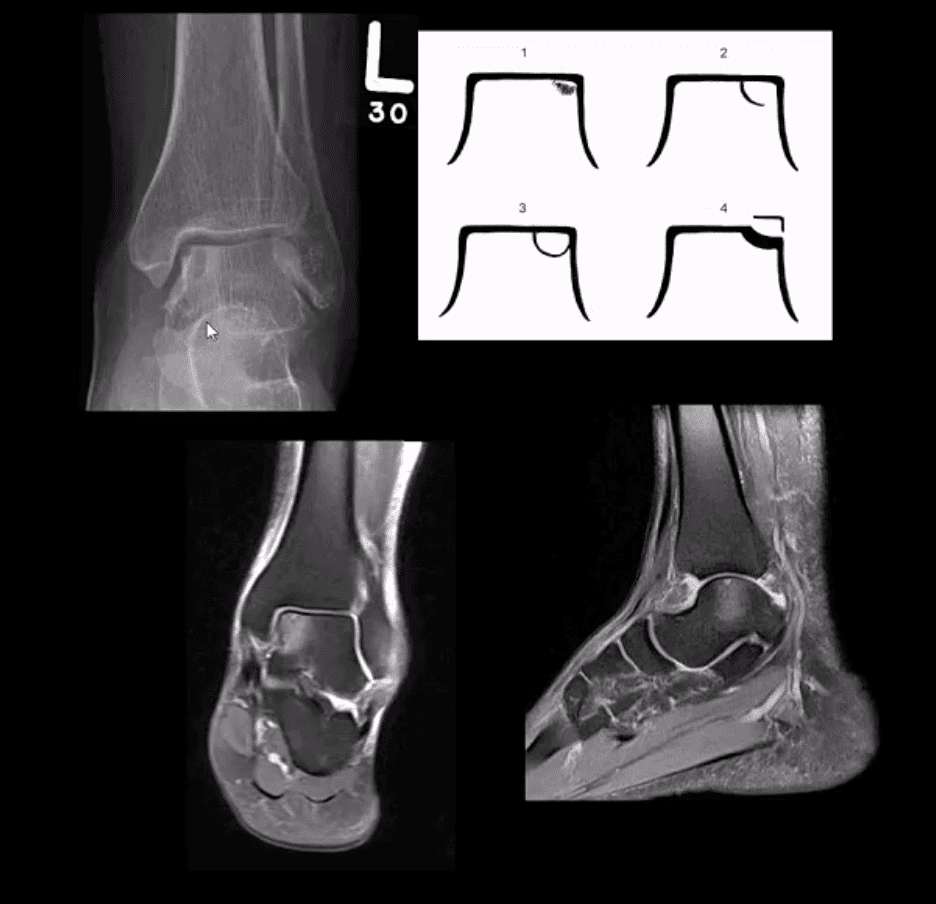
Osteochondral Injury of the Talus (OCD)
Common. Non-traumatic found in superior-medial talar dome. Traumatic may affect supero-lateral dome.
Clinically: pain/effusion/locking. Imaging is crucial.
1st step: radiography may reveal focal radiolucent concavity/halo, fragment.
MRI helpful esp. if OCD is cartilaginous and to demonstrate bone edema.
Jones Fx: extra-articular Fx of proximal metaphysis of the 5th MT. Prone to non-union. Often fixed operatively.
Pseudo-Jones: intra-articular avulsion of 5th MT styloid/base by eccentric contraction of Peroneus Brevis M. Managed conservatively: boot-cast immobilization. Both Jones & Pseudo-Jones Dx by foot series radiography.
Stress Fx. Calcaneus, 2nd, 3rd, 5th MTs. Repeated loading (running) or “March foot” 2nd/3rd MT. Clinically: pain on activity, reduced by rest. Dx: x-rays often unrewarding earlier. MRI or MSK US may help. Managed: Conservatively. Complications; progress into complete Fx
Turf toe: common athletic hyperextension of 1st MTP-sesamoid/plantar plate complex is tearing. 1st MTP unstable/loose. Managed operatively.
Arthritis of the Foot & Ankle
DJD of the ankle: uncommon a primary OA. Typically develops as 2nd to trauma/AVN, RA, CPPD, Hemophilic arthropathy, Juvenile Idiopathic Arthritis, etc. manifests as DJD: osteophytes, JSL, subchondral cysts all seen on x-rays
Inflammatory Arthritis: RA may develop in the ankle or any synovial joint. Will typically presents with symmetrical Hands/feet RA initially (2nd, 3rd MCP, wrists, MTPs in feet) usually with erosion, uniform JSL, juxta-articular osteopenia, and delayed subluxations.
HLA-B27 spondyloarthropathies: commonly affect lower extremity: heel, ankle esp in Reactive (Reiter). Erosive-productive bone proliferation is a crucial Dx.
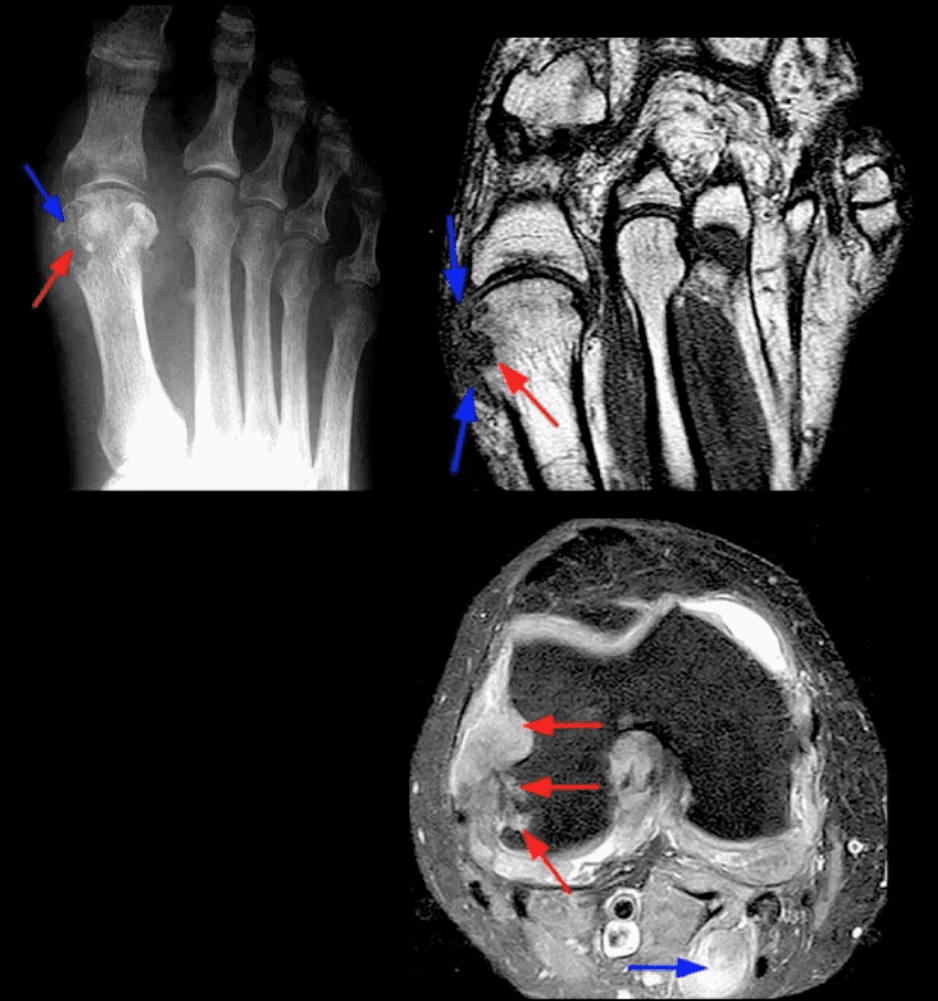
Gouty Arthritis: common in the lower extremity. Ankle, mid-foot foot esp 1st MTPs. Initial onset: acute gouty arthritis with ST effusion and no erosions/tophi. Chronic tophaceous gout: peri-articular, intra-osseous punched-out erosions with over-hanging edges, no initial JSL/osteopenia, ST. Tophi may be seen.
Miscellaneous arthropathy: PVNS. Not common. Affects 3-4th decades of life. The result of synovial proliferation with Macrophages and multi-nucleated Giant Cells filled with hemosiderin and fatty accumulation may lead to inflammation, cartilage damage, extrinsic bone erosions. Dx: x-rays are insensity, MRI modality of choice. Synovial biopsy. Management: operative, can be difficult.
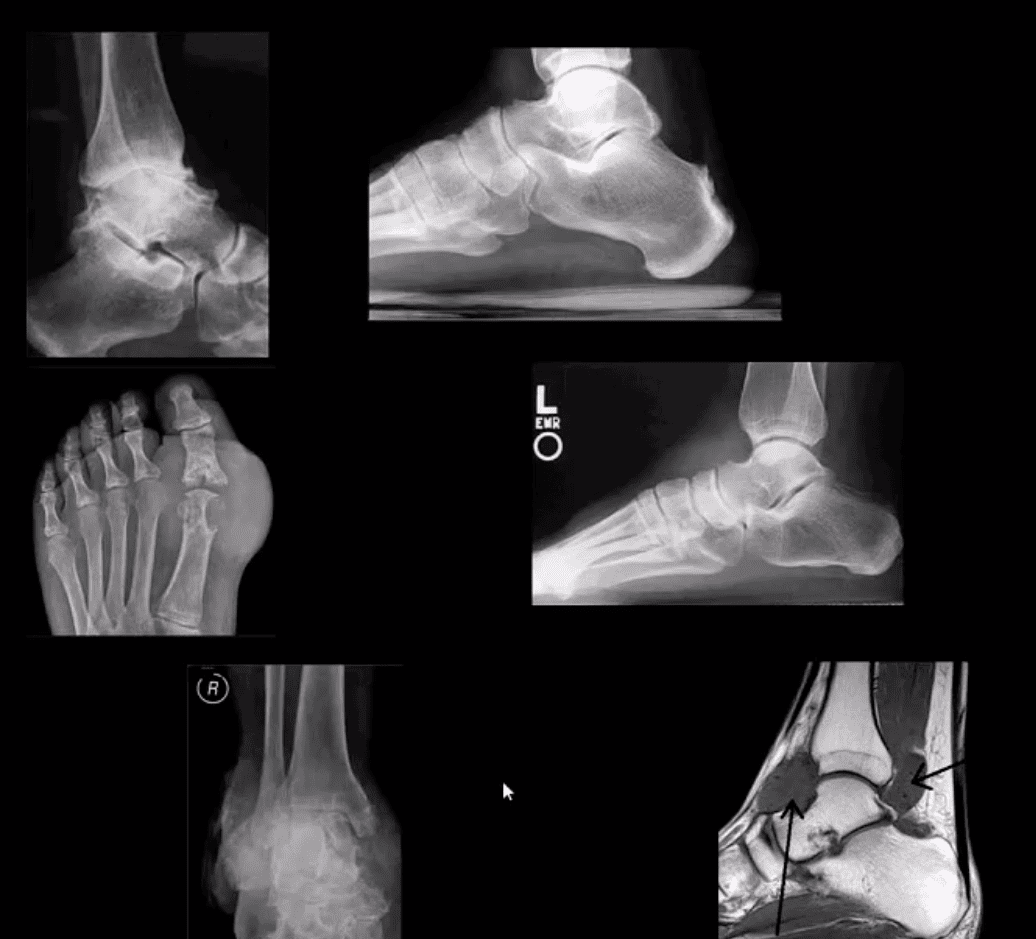
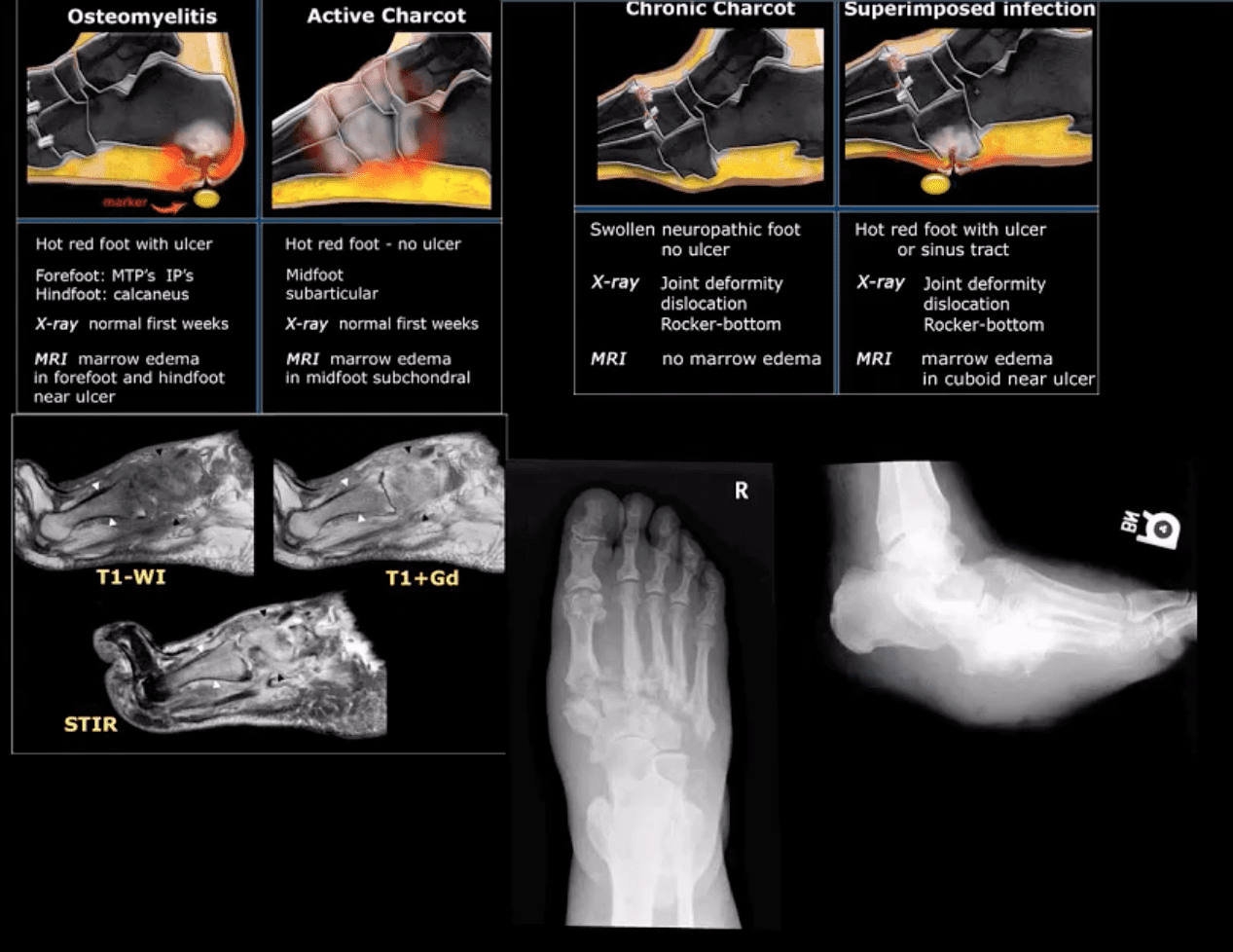
Neuropathic Osteoarthropathy
(Charcot’s joint) Common and on the rise d/t epidemic in type 2 DM. May present with pain initially (50% of cases) and painless destructive arthropathy as a late manifestation. Early Dx: delayed. Imaging is crucial: x-rays: initially unrewarding, some SF effusion is seen. MRI helps with early Dx and extremity off-loading. Late Dx: irreversible dislocations, collapse, disability. Note: Lisfrance dislocation in Charcot joint
M/C mid-foot (TM joint) in 40% of cases, ankle 15%. Progression: Rocker-bottom foot, ulcerations, infections, increased morbidity, and mortality.
Early Dx: by MRI is crucial. Suspect it in patients with type 2 DM especially if early non-traumatic foot/ankle pain reported.
10% of all fractures. 2nd m/c following femoral neck Fx. Demographics: active young males and older osteoporotic females
Stable Fx: overall prognosis is good
Unstable Fx: require ORIF. 15%-20% chances of 2nd OA.
Role of imaging is to determine the complexity, stability and care planning (i.e., operative vs. conservative)
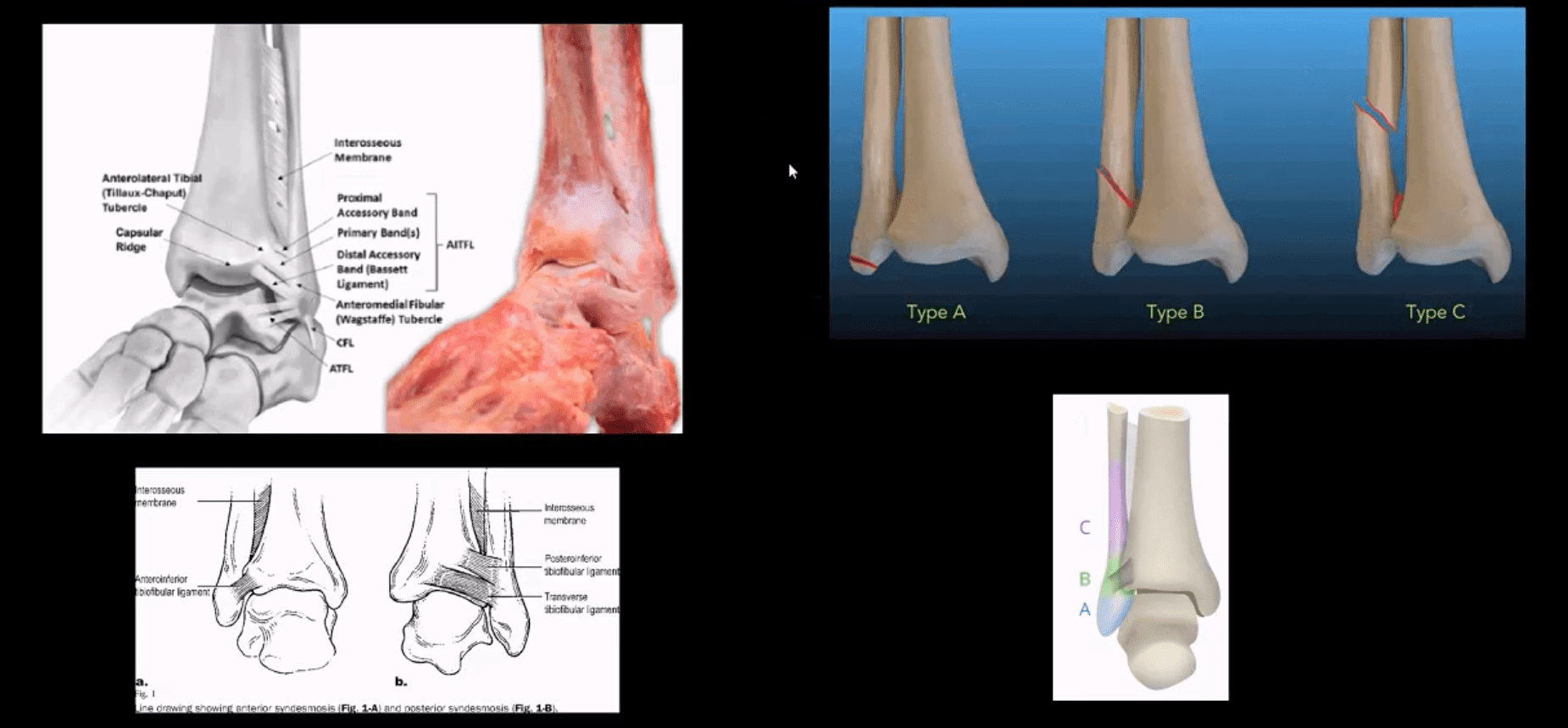
Weber classification considers tearing of distal tibial-fibular syndesmosis and potential instability
Weber A – below syndesmosis. Stable, typically avulsion of the distal fibular malleolus
Weber B – at the level of syndesmosis: may be outside syndesmosis and stable or tearing syndesmosis and unstable
Weber C – above syndesmosis. Always unstable d/t tearing of syndesmosis
Variations of fractures may involve the position/role of the talus bone during Fx (e.g., abduction, adduction, rotation, etc.) this is known as Lauge-Hanson classification
Reveal infrasyndesmotic Fx of fibular malleolus (Weber A)
Stable Injury
Conservative care in the form of short-leg walking cast/boot can be used. Good recovery. If no evidence of osteochondral injury, relatively low chances of post-traumatic OA
No further imaging required. MRI may help to reveal bone contusion and osteochondral injury
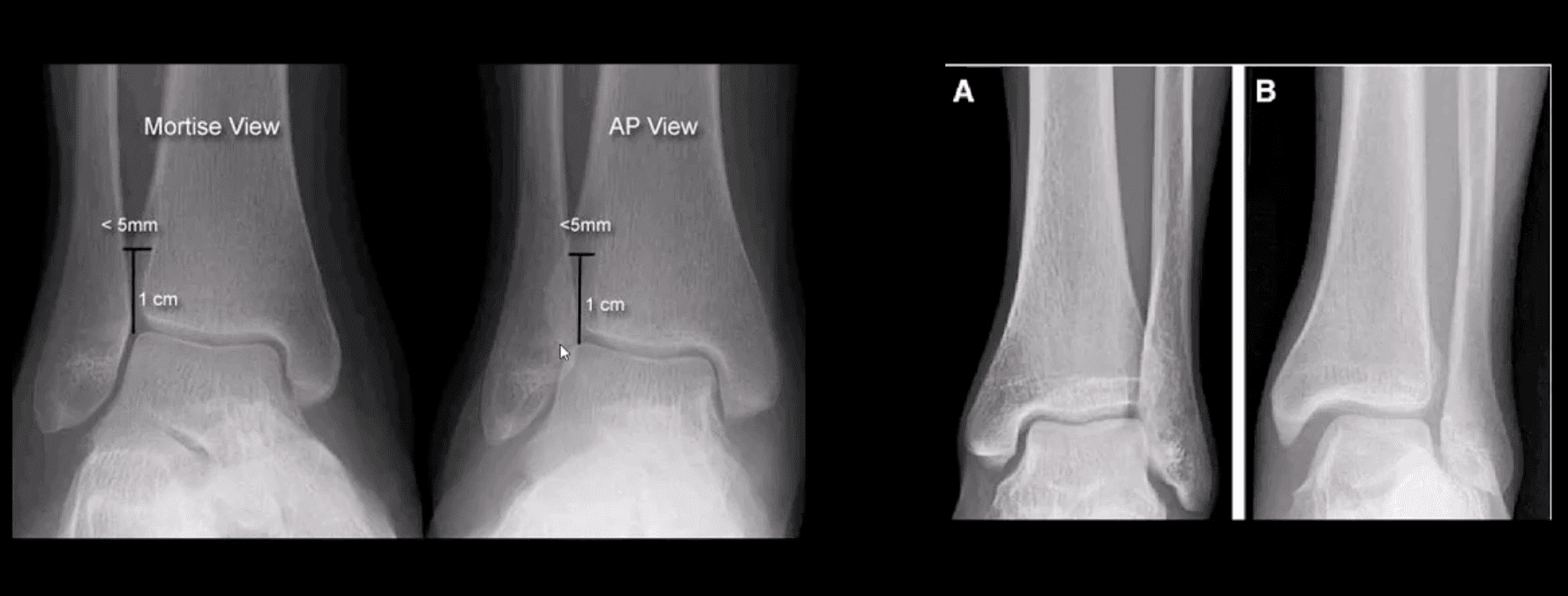
Weber B at Level of Syndesmosis
Can be stable or unstable. On occasions, the decision is made during operative exploration.
CT scanning may help with further evaluation
Management: depends on stability. Additional stabilization required if syndesmosis is ruptured
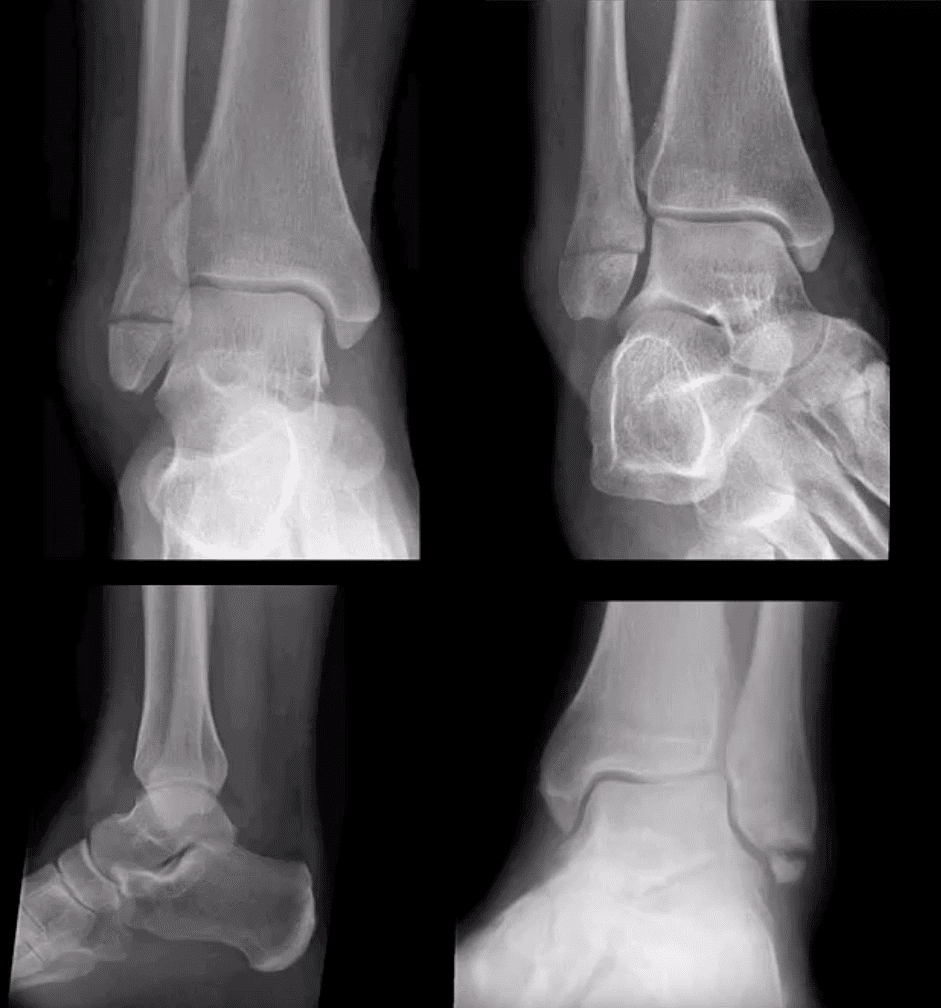
Weber C
AP, medial oblique and lateral views reveal Weber C – suprasyndesmotic injury with abnormal joint widening d/t disruption of the tib-fib syndesmosis. Very unstable injury.
Occasionally, when Weber C Fx positioned 6-cm from the tip of the lateral malleolus, it may be termed as Pott’s ankle Fx (name after Percival Pott’s who has proposed the original classification of ankle fractures based on their stability and degree of rotation). The term is somewhat outdated.
Management: operative with additional stabilization of the syndesmosis
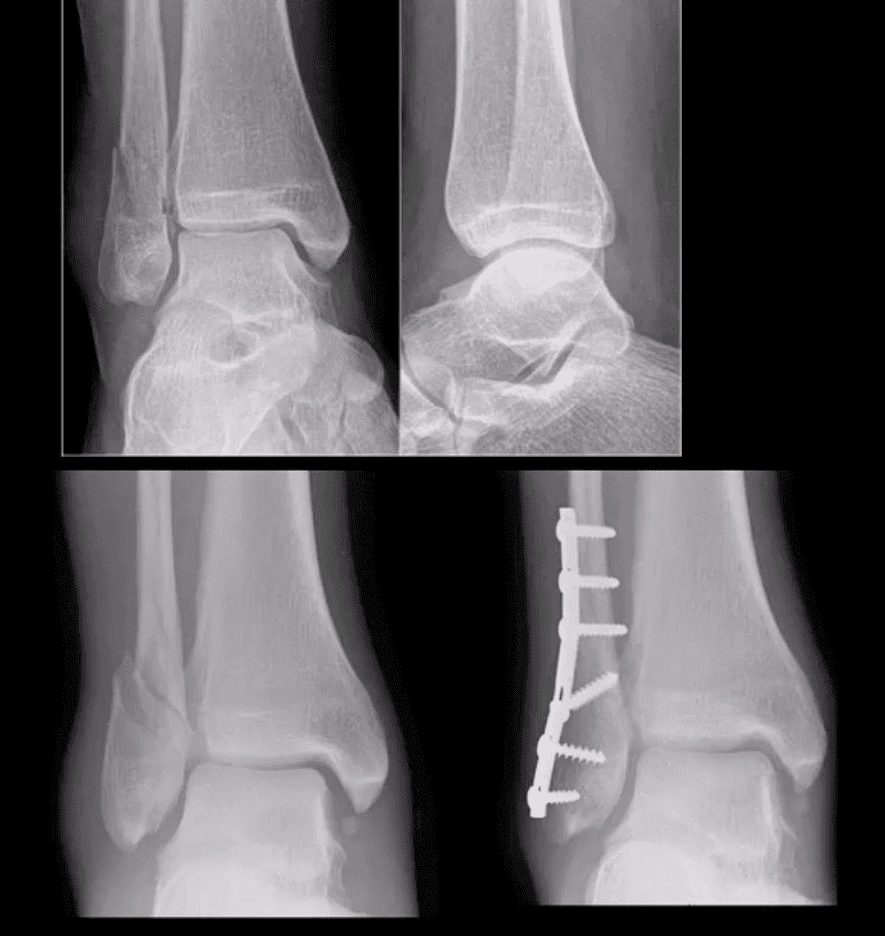
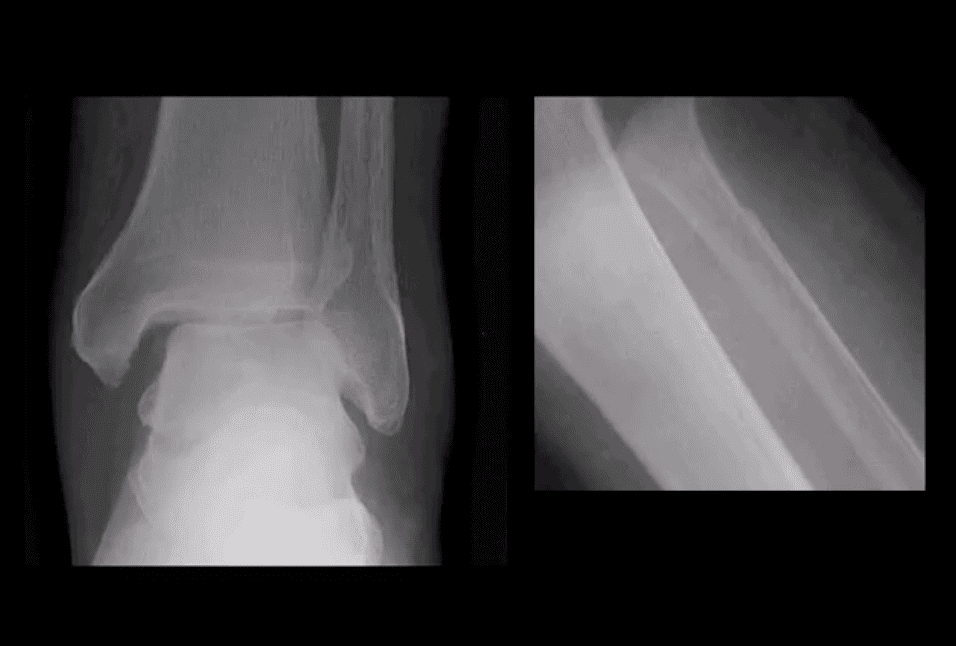
Maisonneuve Fracture
Often spiral fracture of the proximal fibula combined with an unstable ankle injury
No immediate ankle fracture is noted radiographically, thus can be missed on ankle views and require tibia and fibula views
Rad features: widening of the ankle d/t syndesmosis tear and sometimes deltoid ligament disruption. Interosseous membrane is torn with proximal fibular Fx caused by pronation with external-rotation force
Management: operative
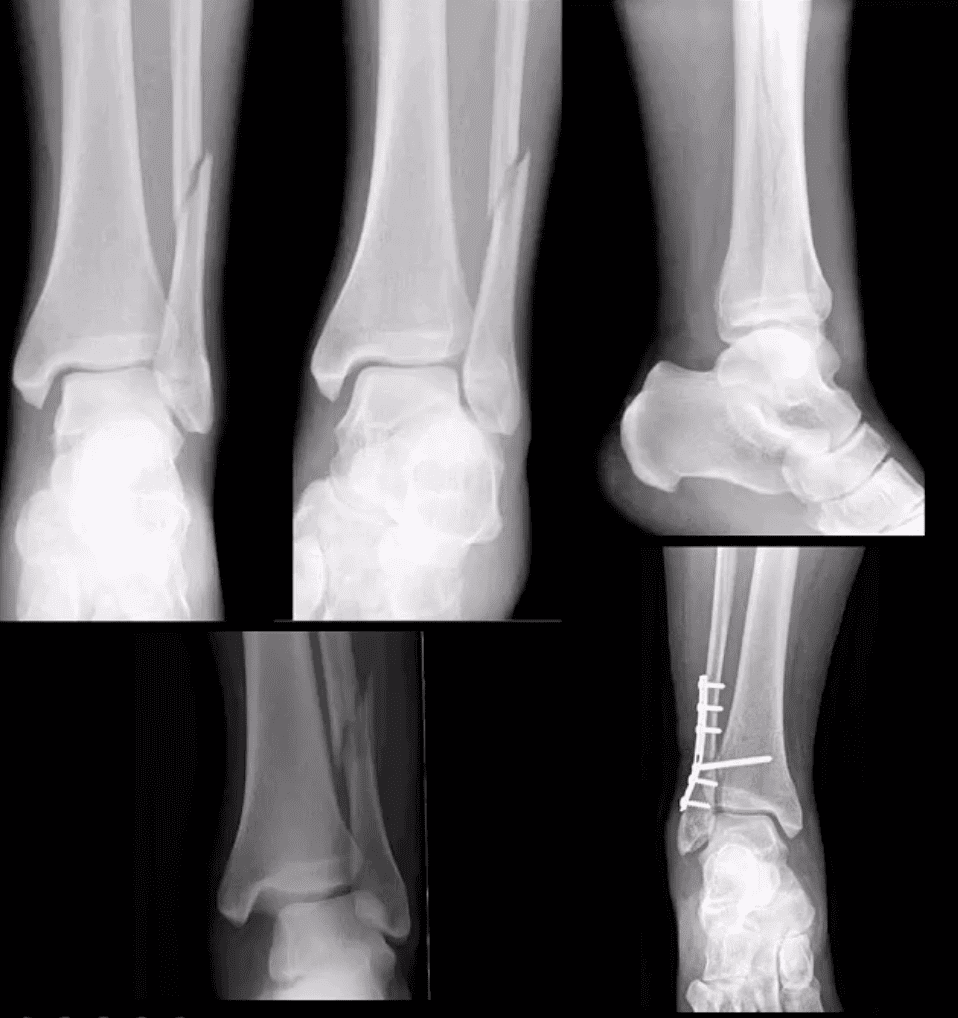
Bimalleolar & Trimalleolar Fx
Above top images Bimalleolar Fx v. unstable, the result of pronation and abduction/external rotation. Rx: ORIF.
Trimalleolar Fx: 3-parts ankle Fx. Medial and lateral malleolus and avulsion of the posterior aspect of tibial plafond. More unstable. Rx: operative
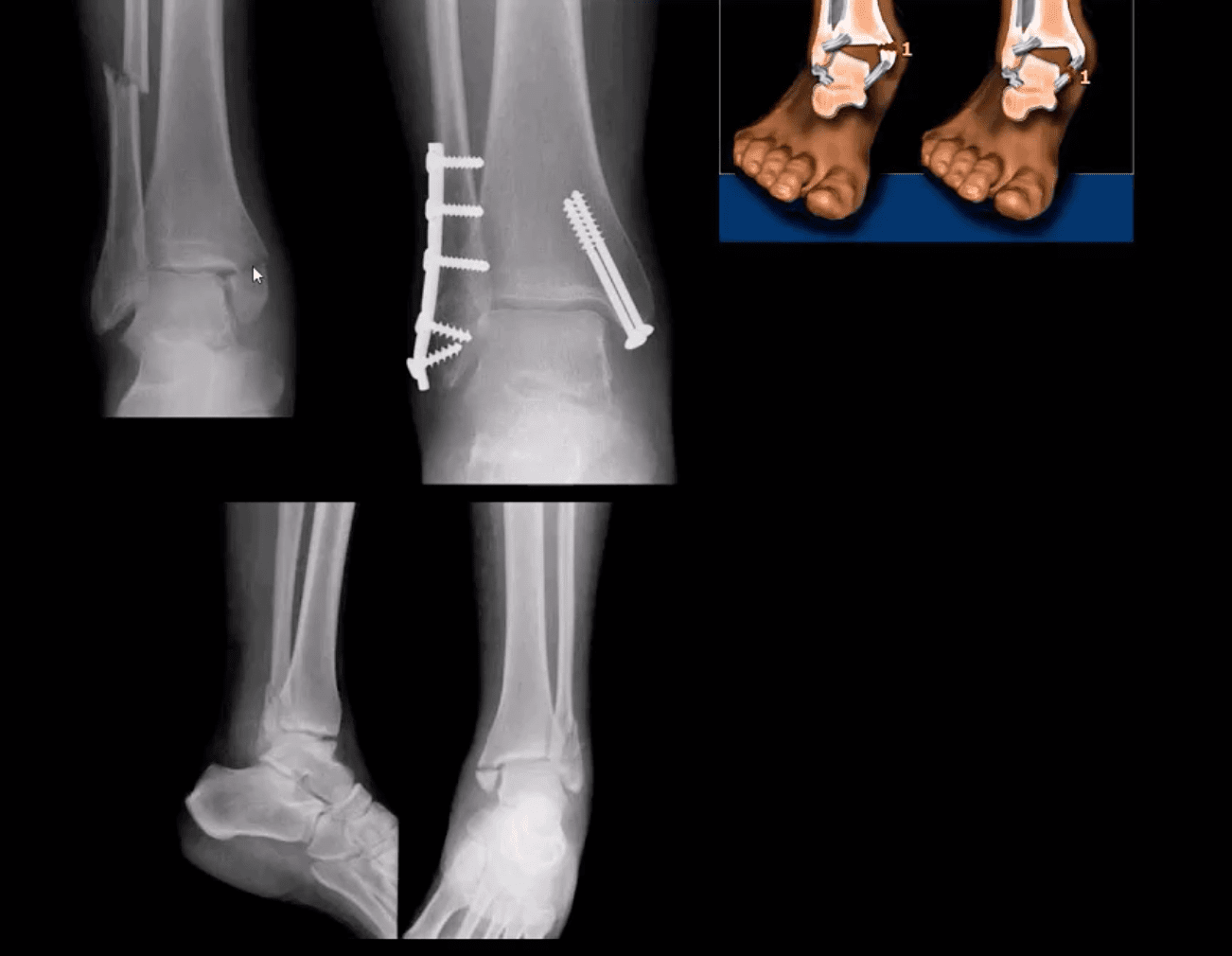
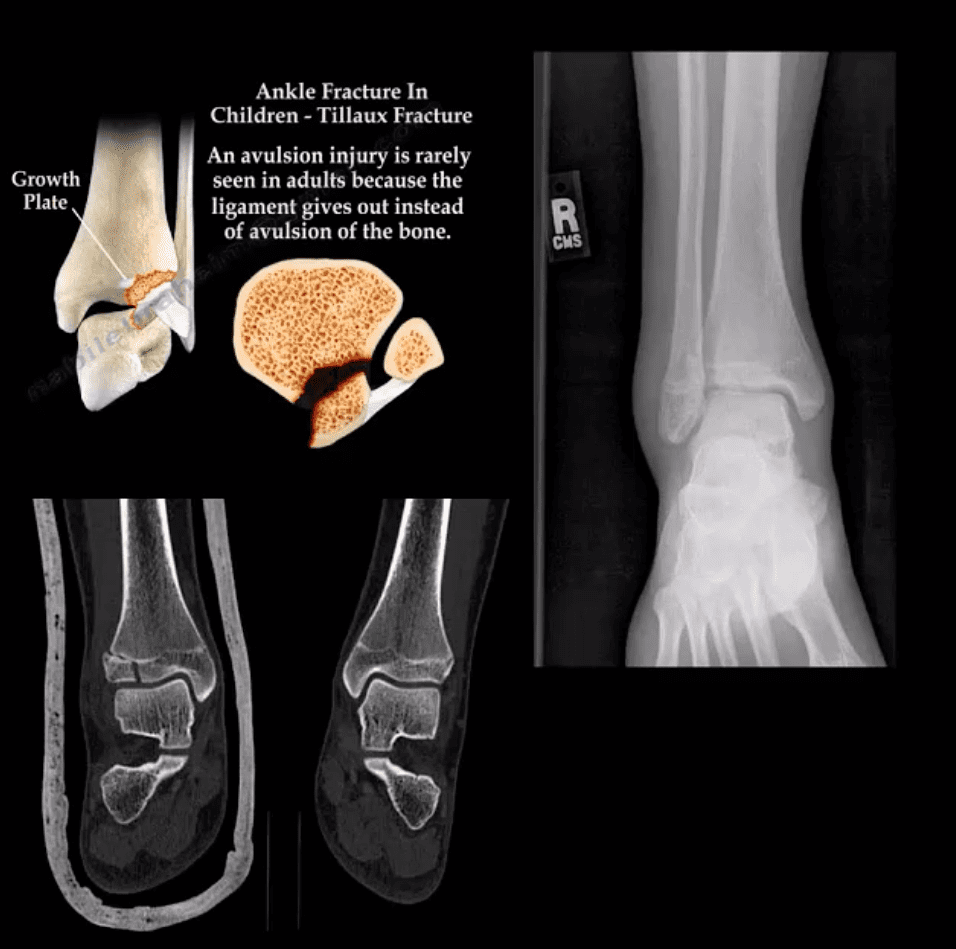
Tillaux Fx
Pediatric Fx affecting older child when the medial side of the physis is closed or about to close with lateral side till open. Avulsion by the anterior tibi-fibular ligament. Complications: 2nd dry/premature OA. Rx: can be conservative if stable by boot cast immobilization.
Pediatric Growth Plate Injuries
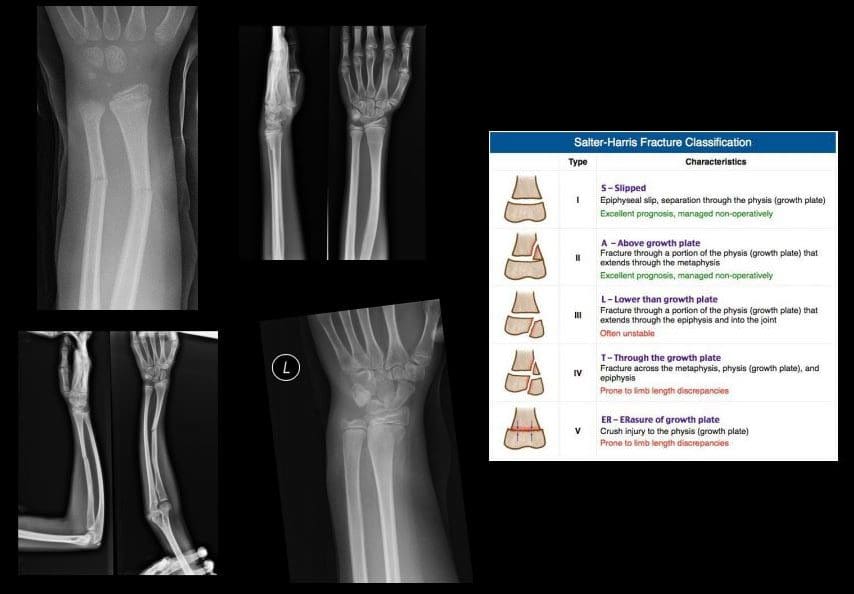
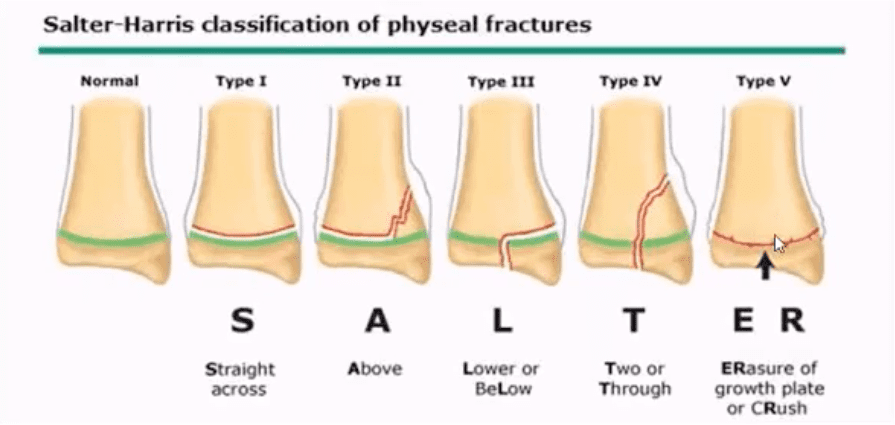
Salter-Harris classification helps to diagnose and prognosticate physeal injuries.
Helpful mnemonic: SALTR
S: type 1-slip through the growth plate
A: type 2-above, Fx extends into the metaphysis
L: type 3-lower, intra-articular Fx extends through the epiphysis
T: type4, “through” Fx extends through all: physis, metaphysis, and epiphysis.
R: type 5, “ruined.” Crush injury to physis leading to complete death of the growth plate
Type 1 and 5: present with no fracture
Type 2: has the best prognosis and considered the most common.
Management: referral to a pediatric orthopedic surgeon
Complications: early physis closure, limb shortening, premature OA and others.
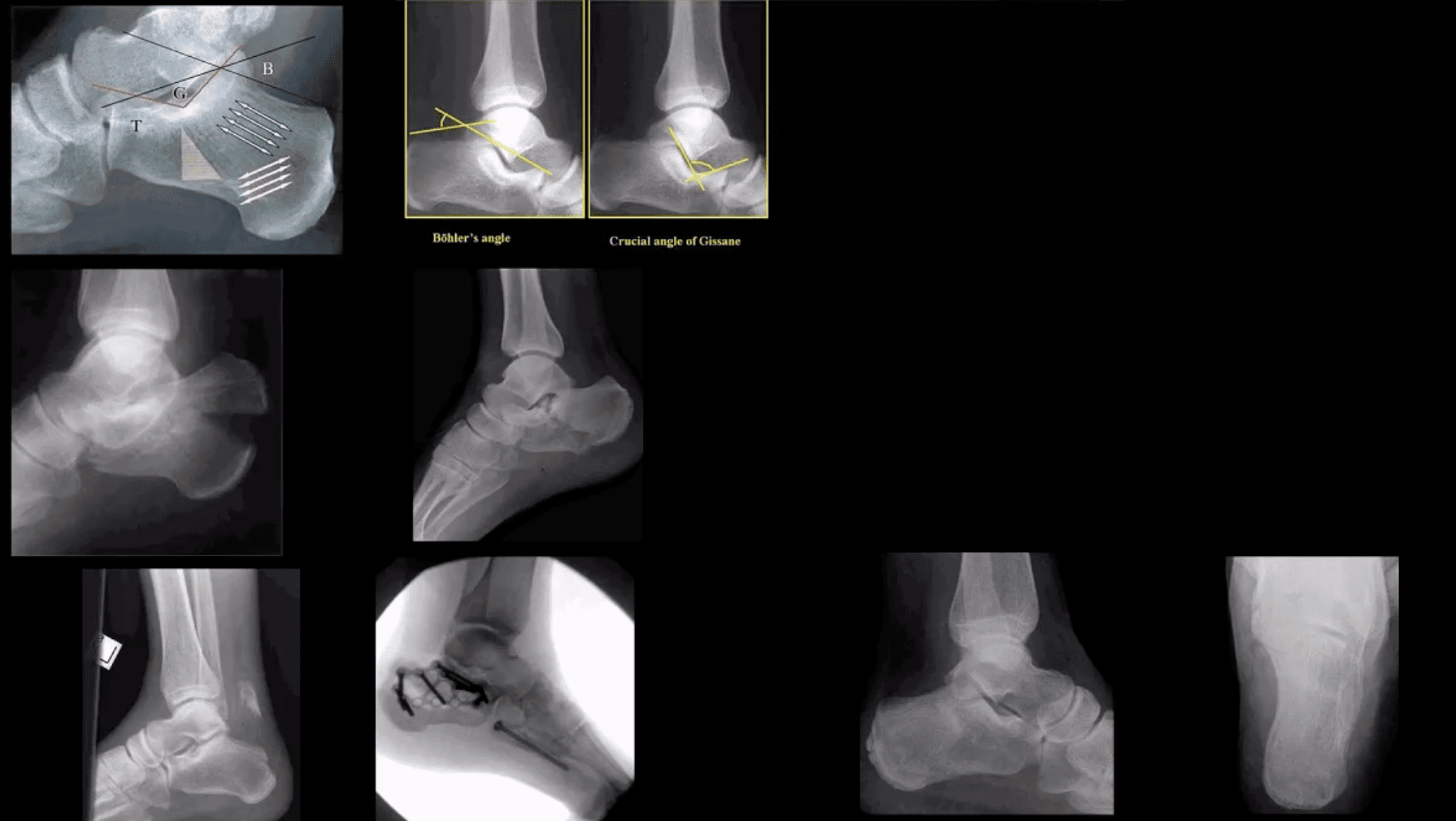
Calcaneal Fracture
Most frequent tarsal Fx. 17% open Fx
Mechanisms: axial loading (intra-articular Fx into sub-talar and calcaneal-cuboid joints in 75% cases). Avulsion by Achilles tendon (m/c in osteoporotic bone). Stress (fatigue) Fx.
Intra-articular Fx carries a poor prognosis. Typically comminuted. Rx: operative.
B/I calcaneal intra-articular fx with associated vertebra compression Fx with associated vertebral compression Fx (T10-L2) often termed Casanova aka Don Juan (Lover’s) fx.
Imaging: x-radiography with added “heel view” 1st step. CT scanning is best for Dx and pre-op planning.
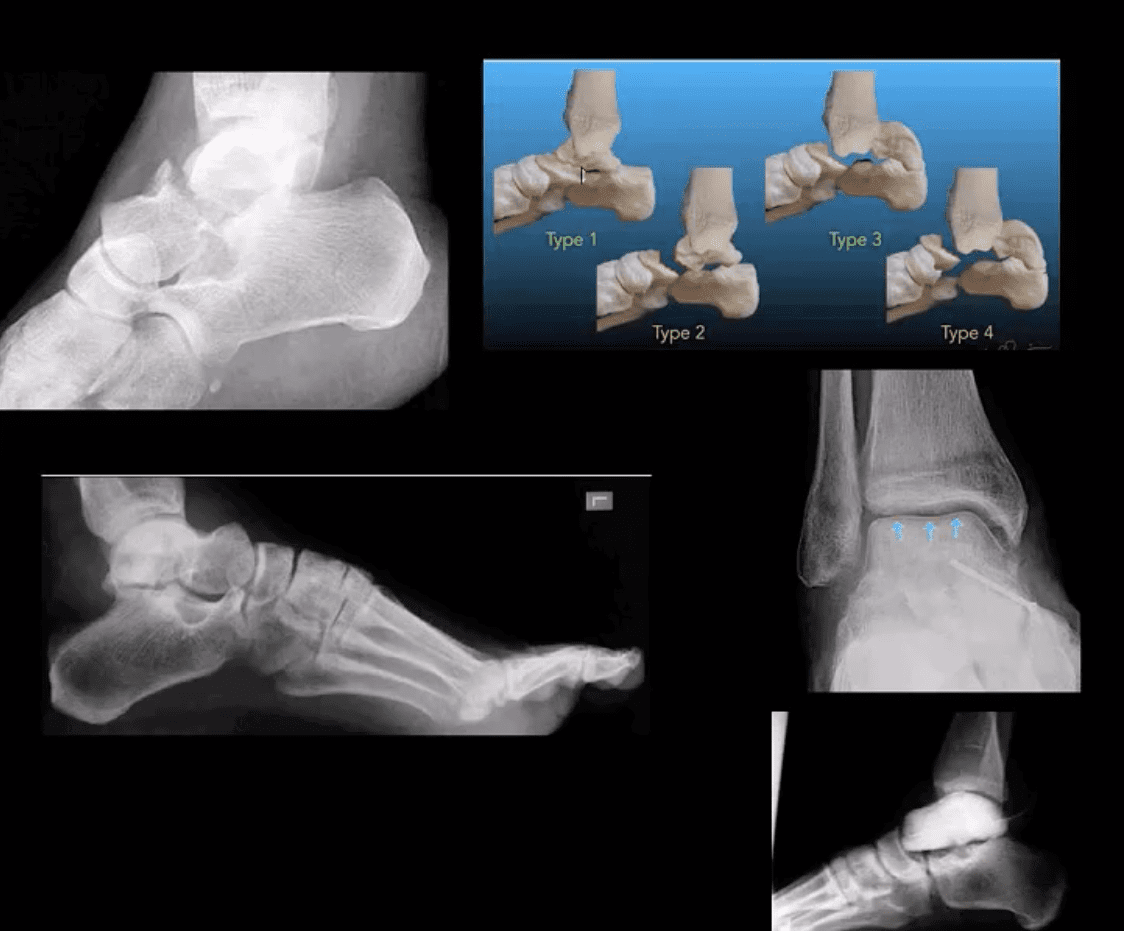
M/C fractured tarsal bone is the Talus. M/C region: talar neck (30-50%). Mechanism: Axial loading in dorsiflexion. Complications: Ischemic osteonecrosis (AVN) of the talus. Premature (2nd OA). Imaging: 1st step: radiographs, CT can be helpful with further delineation
Hawkins classification helps with Dx, prognosis & treatment. “Hawkins sign’ on plain film/CT scan may help with AVN Dx. (above blue arrows indicate good prognosis d/t radiolucent line indicating no AVN because the bone is vascularized and hence resorbed)
Rx: Type 1: conservative with short leg cast or boot (risk of AVN-0-15%), Type 2-4-ORIF (risk of AVN 50%-100%)
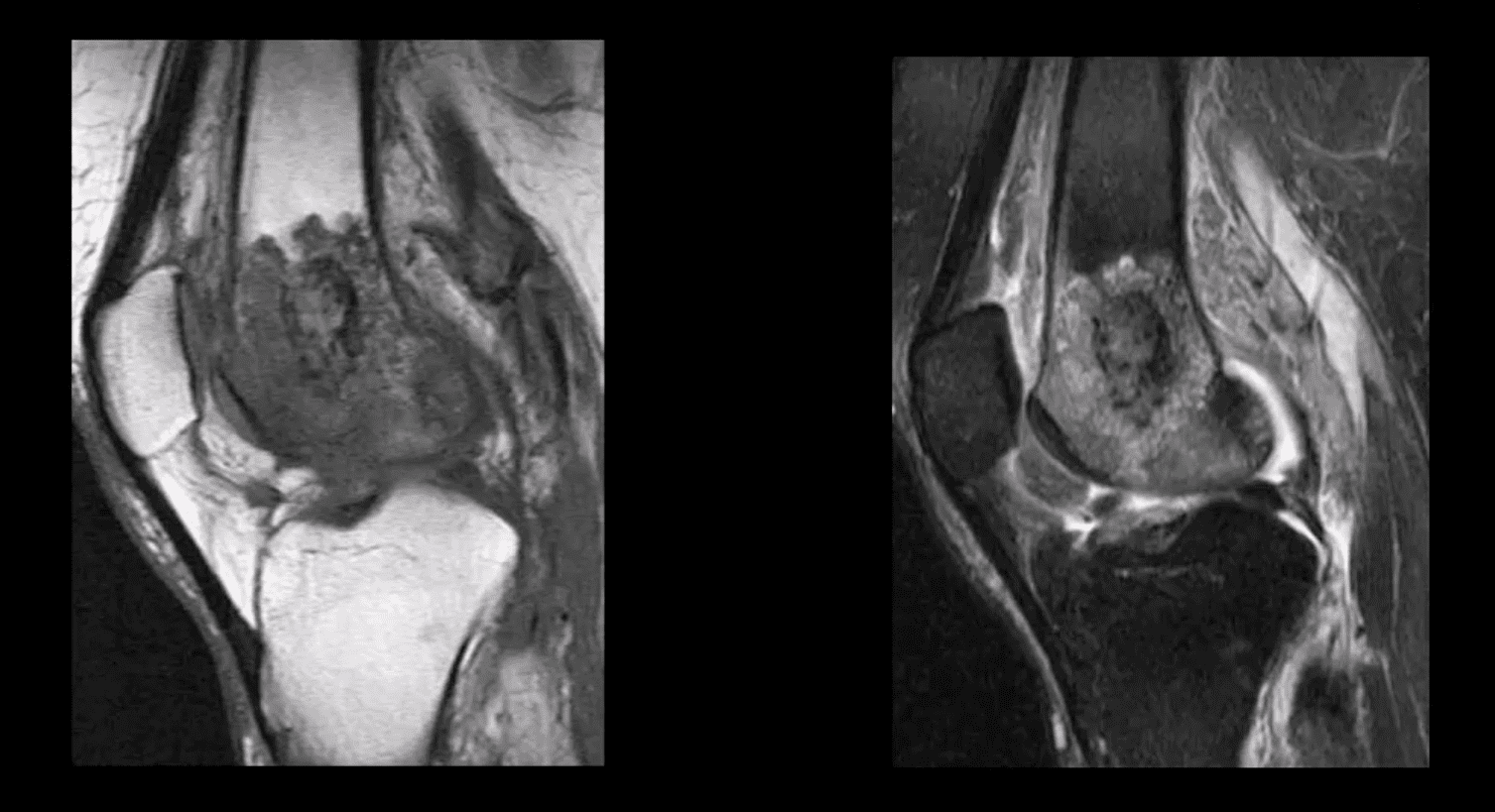
Sagittal Fluid Sensitive MR slice showing large synovial popliteal (Baker’s) cyst (above top image) and sizeable synovial effusion (above bottom image)
Note multiple patchy dark signal areas on both images, representing fibrinoid inflammatory deposits aka “rice bodies” a characteristic MRI feature of RA
Management Rheumatological Referral & DRM
Conservative management followed by operative care in complicated cases of tendon ruptures and joints dislocations
Supplemental reading:
Diagnosis and Management of Rheumatoid Arthritis – AAFP
Septic arthritis – d/t bacterial or fungal contamination of the joint. SA may cause rapid joint destruction and requires prompt Dx and antibiotic administration
Joints affected: large joints with rich blood supply (knee 50%>hips>shoulders).
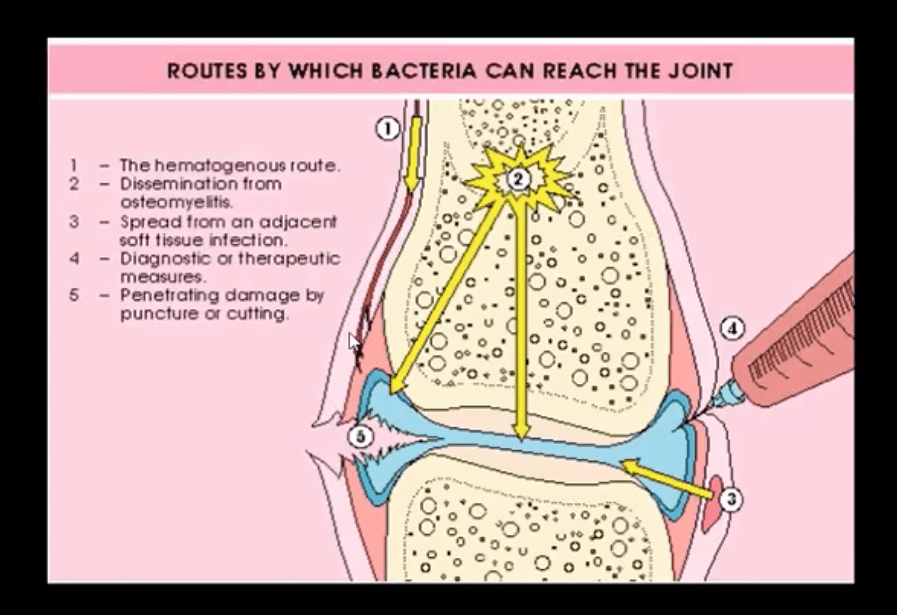
Routs of Infection:
1) Hematogenous is m/c
2) Spread from an adjacent site
3) Direct implantation (e.g., trauma, iatrogenically)
Patients at risk: children, diabetics, immunocompromised, pre-existing joint damage/inflammation, e.g., RA, etc.
I.V. drug users are particularly at risk and also may contaminate atypical joints “the S joints” SIJ, SCJ, Symphysis pubis, ACJ, etc.
Clinically: may vary and depends on host immune response and bacterial virulence. May present with rapid onset or exacerbation of pre-existing joint pain, swelling, limitation of ROM. General signs of malaise, fever, fatigue and elevated ESR, CRP, Leucocytosis may be present.
N.B. Diabetics and immunocompromised may present with fewer manifestations and lack of fever d/t declining immune response
Dx: clinical, radiological and laboratory. Arthrocentesis may be necessary for culture, cell count and purulent synovial examination
Management: I.V. antibiotics
Imaging Dx: begins with radiography but in the early stage most likely will be unremarkable. MRI can be sensitive and help with early identification of joint effusion, bone edema, etc. US may be helpful in the superficial joints and children. US helps with needle guidance. Bone scintigraphy may be used occaisonally if MRI is contraindicated
Routes of Joint Contamination
1. Hematogenous (M/C)
2. Spread from the adjacent site
3. Direct inoculation
M/C organism-Staph aureus
N.B Gonococcal infection may be a top differential in some cases
IV drug users: Pseudomonas, candida
Sickle cell: Salmonella
Animal (cats/dogs) bites: Pasteurella
Occasionally fungal contamination may occur
Radiography
Initially non-specific ST/joint effusion, obscuration/distortion of fat planes. Because it takes 30% of compact and 50-75% trabecular bone to be destroyed before seen on x-rays, radiography is insensitive to some of the early changes. MR imaging is the preferred modality
If MRI is not available or contraindicated. Bone scintigraphy with Tc-99 MDT can help
In children, US preferred to avoid ionizing radiation. In children, US can be more sensitive than in adults due to lack of bone maturation
Radiographic Dx
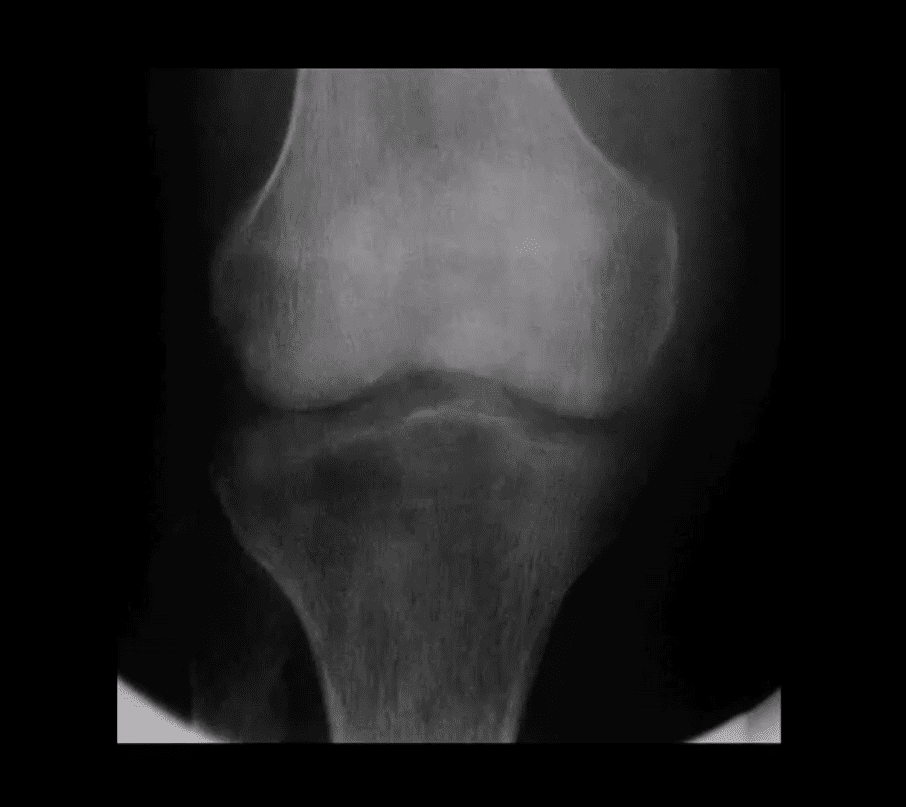
Early findings are unrewarding. Early features may include joint widening d/t effusion. Soft tissue swelling and obscuration/displacement of fat planes
1-2 weeks: periarticular and adjacent osseous changes are manifesting as patchy demineralization, moth-eaten, permeating bone destruction, loss, and indistinctness of the epiphyseal “white cortical line” with an increase in soft tissue swelling. MRI may be helpful with early Dx.
Late features: complete joint destruction and ankyloses
N.B. Septic arthritis may progress rapidly within days and requires early I.V. antibiotic to prevent major joint destruction
T1 & T2 Knee MRI
T1 (above left) and T2 fat-sat sagittal knee MRI slices reveal loss of normal marrow signal on T1 and increase on T2 due to septic edema. Bone sequestrum d/t osteomyelitis progressing into septic arthritis is noted. Marked joint effusion with adjacent soft tissue edema is seen. Dx: OSM and septic arthritis
Imaging may help the Dx of the septic joint. However, the final Dx is based on Hx, physical examination, blood tests and most importantly synovial aspiration (arthrocentesis)
Synovial fluid should be sent for Gram staining, culture, glucose testing, leukocyte count, and differential determination
ESR/CRP may be elevated
Synovial fluid: WBC can be 50,000-60,000/ul, with 80% neutrophils with depleted glucose levels Gram stain: in 75% gram-positive cocci. Gram staining is less sensitive in gonococcal infection with only 25% of cultures +
In 9% of cases, blood cultures are the only source of pathogen identification and should be obtained before antibiotic treatment
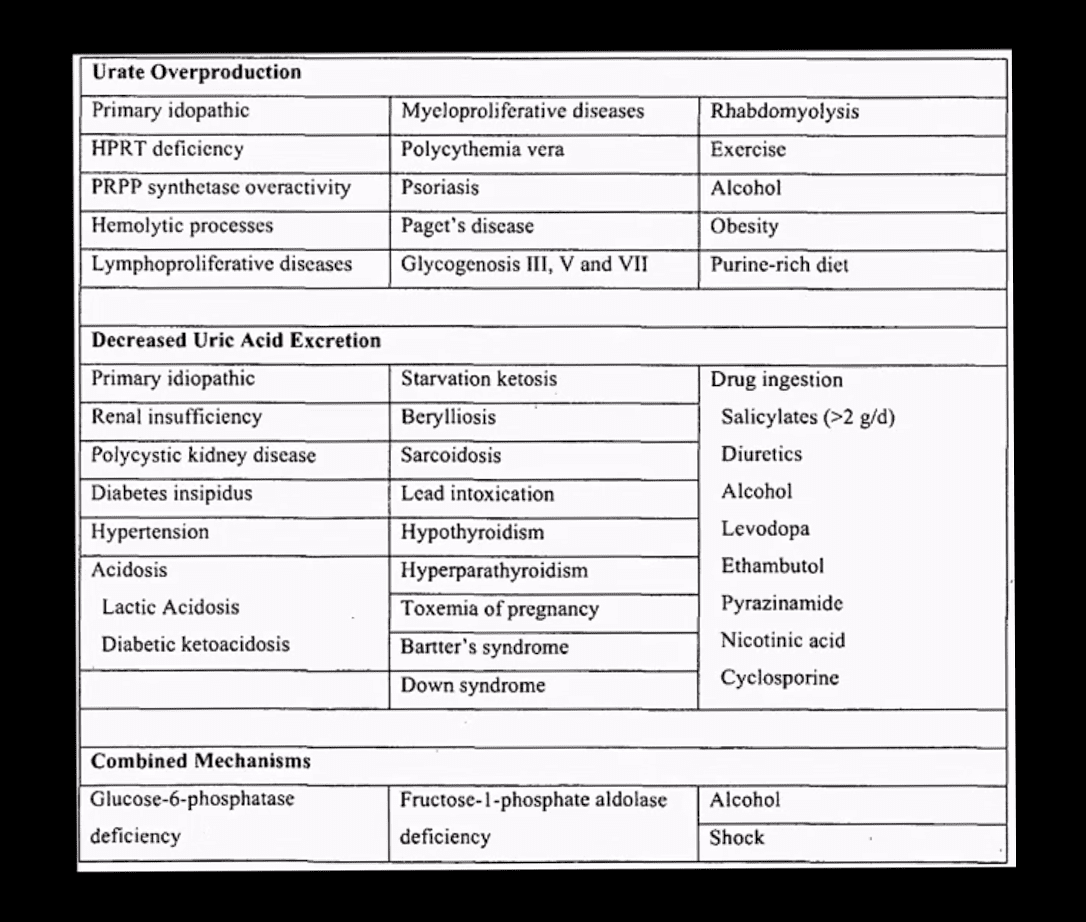
Gout: MSU deposition in and around joints and soft tissues. Elevated levels of serum uric acid (UA) (>7mg/dL) caused by overproduction or under-excretion of uric acid
Once UA reached/exceeded 7mg/dL, it will deposit in the peripheral tissues. Primary gout: disturbed metabolism of nucleic acids and purines break down. Secondary gout: increased cell turnover: Psoriasis, leukemia, multiple myeloma, hemolysis, chemotherapy, etc.
Gout presents with 5-characteristic stages:
1)asymptomatic hyperuricemia (years/decades)
acute attacks of gouty arthritis (waxes and wanes and lasts for several years)
Interval phase between attacks
Chronic tophaceous gout
Gouty nephropathy
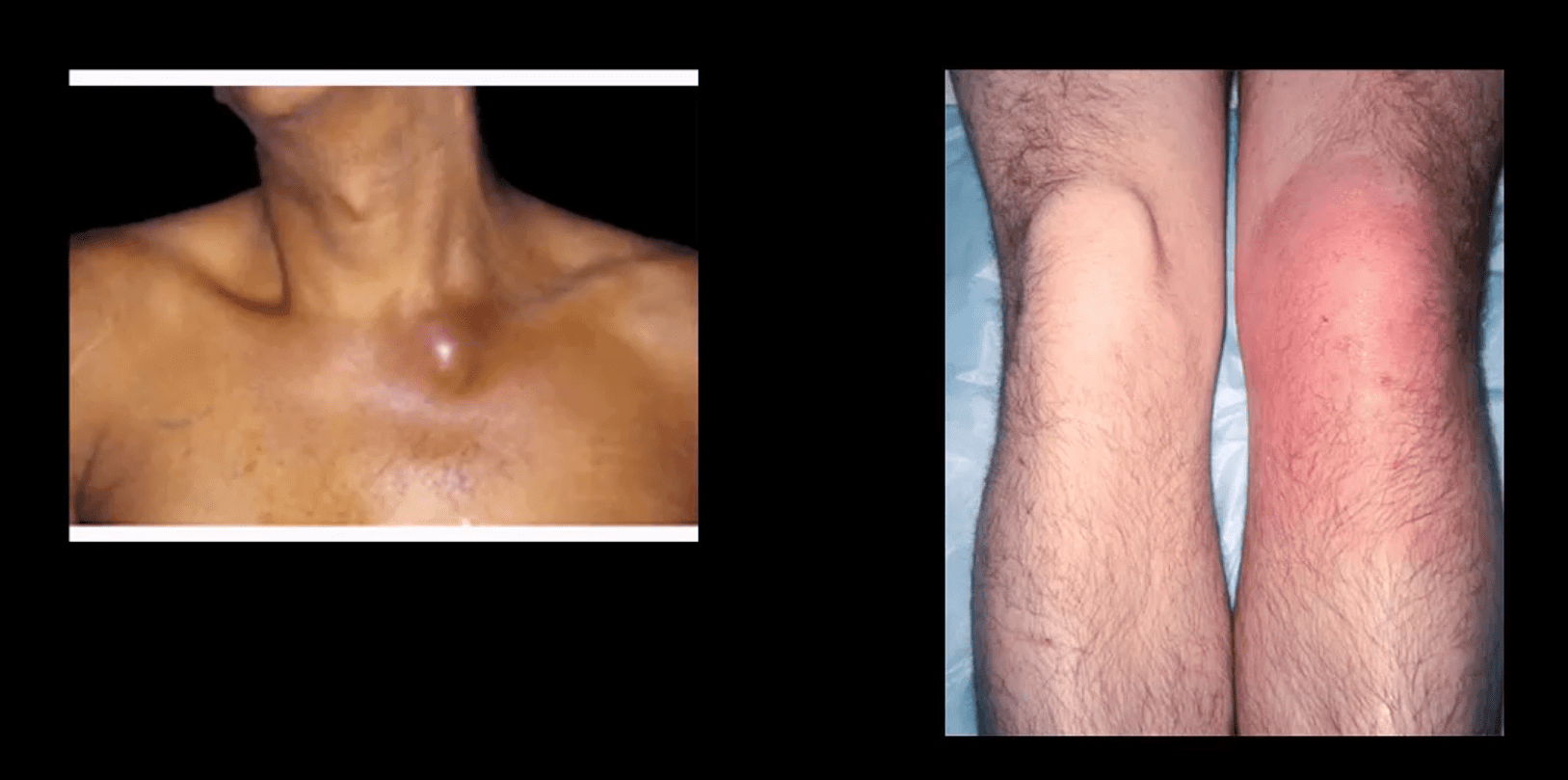
Clinical Presentation
Depends� on stages
Acute attacks: acute joint pain “first and the worst” even painful to light touch
DDx: septic joint (both may co-exist) bursitis etc.
Gouty arthritis typically presents as monoarthropathy
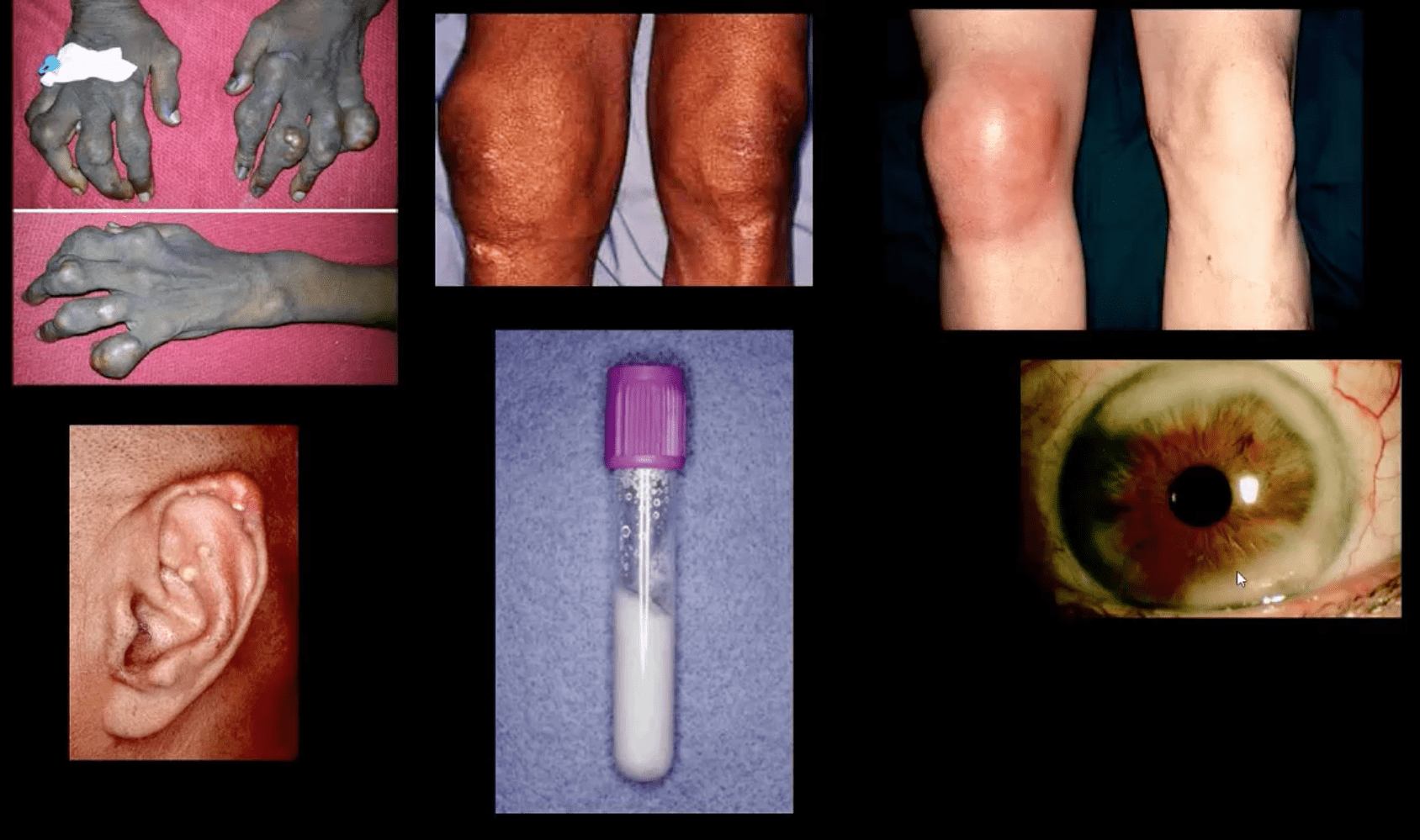
Chronic tophaceous stage: deposits in joints, ear pinna, ocular structures, and other regions. Nephrolithiasis etc. Men>women. Obesity, diet, and age >50-60.
Radiography: early attacks are unremarkable and may present as non-specific joint effusion
Chronic tophaceous gout radiography: punched out peri-articular, para-articular and intraosseous erosions with overhanging edges. A characteristic rim of sclerosis and internal calcification, soft tissue tophi. Target sites: lower extremity m/c
Rx: allopurinol, colchicine (esp. preventing acute episodes and maintenance)
Synovial Aspiration
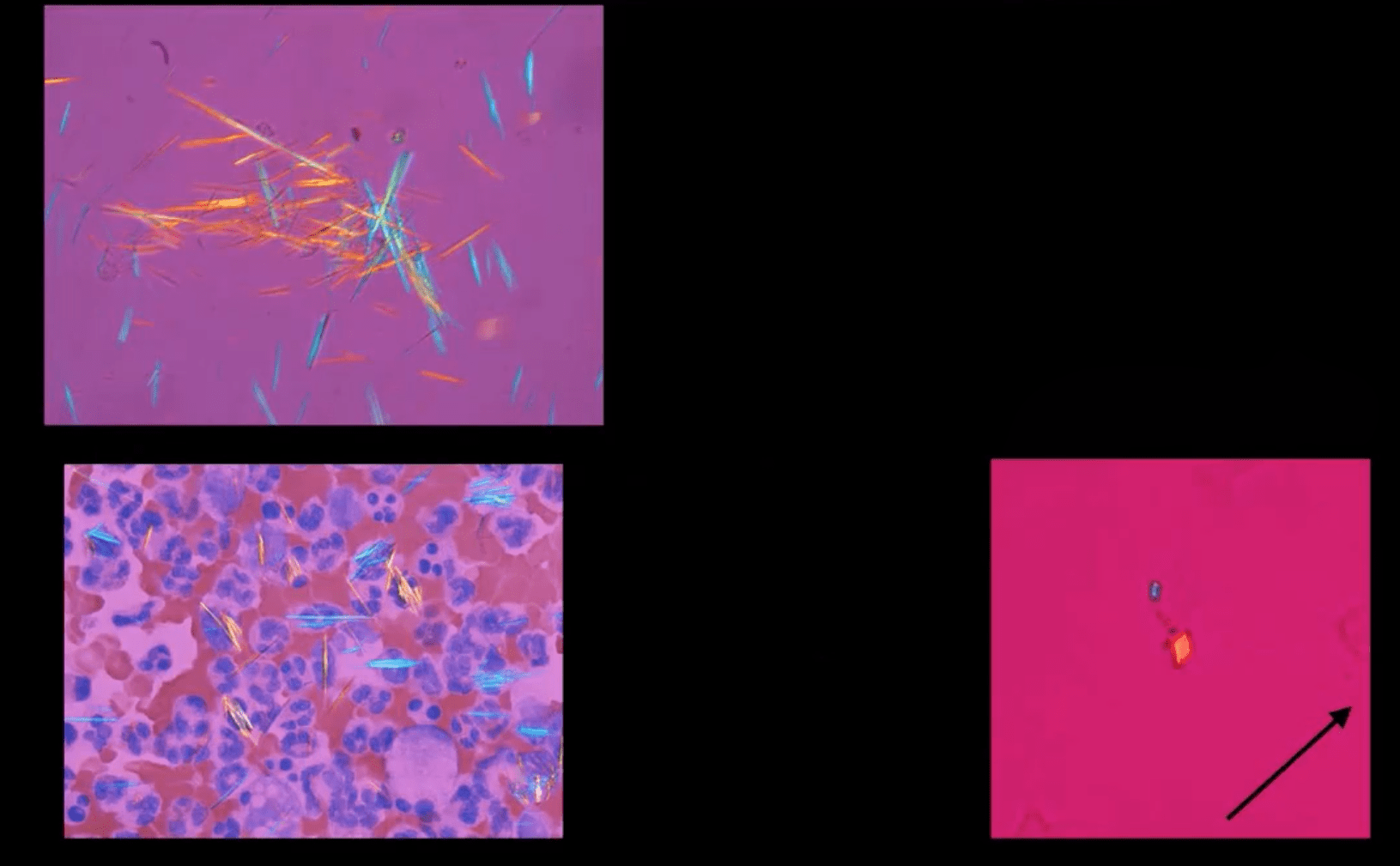
Synovial aspiration with polarized microscopy reveal negatively birefringent needle-shaped MSU crystals with large inflammatory PMN presence. DDx: positively birefringent rhomboid-shaped CPPD crystals (above bottom right) seen in Pseudogout and CPPD
Large S.T.
Density and joint effusion punched out osseous erosion with overhanging margins, overall preservation of bone density, internal calcifications Dx: chronic tophaceous gout
MRI Gout Features
Erosions with overhanging margins, a low signal on T1 and high on T2 and fat-suppressed images. Peripheral contrast enhancement of tophaceous deposits d/t granulation tissue
Dx: final Dx; synovial aspiration and polarized microscopy
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine