Healthy Posture Guidelines: Posture is how an individual holds their body. Healthy posture is when minimal stress is applied to the joints. Maintaining and holding your body correctly can prevent pain, injuries, and other health problems. Faulty postures and musculoskeletal imbalances often precipitate painful conditions in the spine and extremities. However, unhealthy postures do not always present with discomfort and pain symptoms that can go unnoticed for years. This leads to chronic stress and advanced wear of the joints. Injury Medical Chiropractic and Functional Medicine Clinic can realign the spine, relieve symptoms, and restore flexibility, mobility, and function.
Healthy Posture Guidelines
There are two types of posture:
Dynamic Posture
This posture is when the body moves, like walking, running, or bending to pick up something.
Static Posture
This posture is when the body is not moving, like sitting, standing, or sleeping.
Both are important, and the key is the spine’s position. The spine has three natural curves: neck, mid, and low back. Correct posture maintains the curves with the head above the shoulders, and the top of the shoulder should be over the hips.
Unhealthy Positioning
Postural faults include:
Forward head positioning
Rounded shoulders
Loss of the normal lordosis curve in the lower back.
Early warning signs of postural problems may include:
The inability to sit or stand for a prolonged period.
Stiffness when getting up from a chair after sitting.
Feeling of physical exhaustion at the end of the day.
Muscle imbalances.
Loss of normal flexibility.
Symptoms of discomfort.
Affected Health
Unhealthy posture can affect overall health and includes:
Misaligned musculoskeletal system.
Decreased flexibility.
Neck, shoulder, and back pain.
The advanced wearing down of the spine making it more fragile and susceptible to injury.
Affected joint movement.
Affected balance.
Increased risk of falling.
Digestion problems.
Potential breathing problems.
Improvements
Be mindful of your posture during everyday activities, like walking, watching tv, washing dishes, etc.
Maintain Physical Activity
Certain exercises like yoga, tai chi, and other classes focusing on body awareness can help develop healthy posture habits.
Exercises that strengthen the core muscles around the back, abdomen, and pelvis.
Maintain Healthy Weight
Extra weight can weaken the abdominal muscles, cause problems for the pelvis and spine, and contribute to back pain.
Wear Comfortable Shoes
High heels, for example, can throw off the body’s balance and force unhealthy walking movements.
This puts added stress on the muscles and affects posture.
Proper Height
Make sure workstations are at a comfortable height, whether sitting in front of a computer, making dinner, or eating.
Chiropractic Care
Chiropractors and physical massage therapists specialize in evaluating and treating musculoskeletal dysfunction and identifying and screening for postural dysfunction. Healthy posture can have an immediate effect on health that include:
Proper alignment of bones and joints.
Reduced wear on the muscles and joints.
Reduced stress on ligaments.
Decreased risk of back injury.
Increased energy.
Improved digestion.
A chiropractic team will massage and relax the muscles reducing tension, adjust and realign the spine, increase joint movement, and ease the individual into a healthy posture. The team will also provide careful rehabilitation exercises and nutritional recommendations to maintain a healthy posture.
Custom Foot Orthotics
References
Carini, Francesco, et al. “posture and posturology, anatomical and physiological profiles: overview and current state of the art.”Acta bio-medica : Atenei Parmensis vol. 88,1 11-16. 28 Apr. 2017, doi:10.23750/abm.v88i1.5309
Creze, Maud, et al. “posture-related stiffness mapping of paraspinal muscles.”Journal of anatomy vol. 234,6 (2019): 787-799. doi:10.1111/joa.12978
Korakakis, Vasileios, et al. “physiotherapist perceptions of optimal sitting and standing posture.”Musculoskeletal science & practice vol. 39 (2019): 24-31. doi:10.1016/j.msksp.2018.11.004
Many individuals do not realize the importance of the type of pillow they use for sleep. Sleeping on the wrong pillow is the perfect set-up for neck, shoulder, and back pain. Here are a few chiropractic tips on what to know about picking the best pillow. Knowing which is the right pillow for you can be the key to proper sleep and waking up pain-free.
Importance of Pillows
Neck and shoulder pain can be a nightmare, especially when the body cannot get decent rest. The right pillow/s can help with neck and back pain symptoms and recover from injuries quicker. When the head is in an awkward position for sleep duration, this causes neck, shoulder, and headache problems. The importance of finding the right pillow follows a set of guidelines.
Shape
The shape of the pillow has a definitive role in the cervical/neck’s curvature.
Posture
Sleep posture is important in preventing neck, shoulder, and back musculoskeletal pain.
Sleep quality
Craniocervical pressures and cervical spine alignment are height-specific. Any changes can affect an individual’s sleep quality.
Height
Cervical alignment can become significantly impacted by the shape and height of the pillow.
Pillow Comfort Importance
Trying to find the right pillow will require trial and error. The basics to consider include:
One sign that it’s time for a new pillow is waking up with pain.
Age of current pillows. The recommendation is they should be replaced every year or two. This depends on the stuffing/material used as different types wear down quicker.
If problems are getting comfortable and being able to fall asleep.
Constantly readjusting or fluffing the pillow/s.
The pillow has become lumpy or lost its shape.
It is flat with no cervical support or, too high placing the head in a forward tilt.
This is an online quiz along with a personalized process in their stores.
The process helps choose a pillow based on individual support preferences and sleep position for the best spinal alignment.
Customizable or adjustable pillows are another option. These pillows allow the individual to change the amount of filling to fit their needs.
Research, personal preference, and advice from a doctor and or chiropractor will help find the pillow that is right for you.
A third of an individual’s life is spent in bed. Make it as comfortable as possible.
Body Health
Sleep Body Composition Importance
Not getting enough sleep makes it difficult to gain muscle.
Not getting enough sleep means that the body experiences less short wave sleep, affecting the body’s ability to secrete Growth Hormone and develop muscle.
Testosterone is negatively affected by lack of sleep.
Not enough sleep increases cortisol levels, impairing muscle development.
Not getting enough sleep makes it difficult to lose fat.
Irregular sleep throws off the body’s ghrelin/leptin cycles, causing hunger.
Not getting enough sleep has been linked to eating more.
Not getting enough sleep can cause reductions in the body’s Basal Metabolic Rate, reducing total energy output.
“Effect of pillow height on the biomechanics of the head-neck complex: investigation of the craniocervical pressure and cervical spine alignment.” PeerJ. August 2016. pubmed.ncbi.nlm.nih.gov/27635354/
“Improving the quality of sleep with an optimal pillow: a randomized, comparative study.” Tohoku Journal of Experimental Medicine. July 2014. pubmed.ncbi.nlm.nih.gov/25008402/
“The effects of pillow designs on neck pain, waking symptoms, neck disability, sleep quality and spinal alignment in adults: A systematic review and meta-analysis.” Clinical Biomechanics. May 2021. pubmed.ncbi.nlm.nih.gov/33895703/
Okamoto-Mizuno, Kazue, and Koh Mizuno. “Effects of thermal environment on sleep and circadian rhythm.” Journal of physiological anthropology vol. 31,1 14. 31 May. 2012, doi:10.1186/1880-6805-31-14
Low back pain represents one of the most common complaints in healthcare settings. While various injuries and conditions associated with the musculoskeletal and nervous system can cause low back pain, many healthcare professionals believe that work injury may have a prevalent connection to low back pain. For instance, improper posture and repetitive movements may often cause work-related injuries. In other cases, environmental accidents at work may cause work injuries. In any case, diagnosing the source of a patient’s low back pain to correctly determine which would be the best treatment method to restore the individual’s original health and wellness is generally challenging.
First and foremost, getting the right doctors for your specific source of low back pain is essential for finding relief from your symptoms. Many healthcare professionals are qualified and experienced in treating work-related low back pain, including doctors of chiropractic or chiropractors. As a result, several work injury treatment guidelines have been established to manage low back pain in healthcare settings. Chiropractic care focuses on diagnosing, treating, and preventing various injuries and conditions, such as LBP, associated with the musculoskeletal and nervous system. By carefully correcting the misalignment of the spine, chiropractic care can help improve symptoms of low back pain, among other symptoms. The purpose of the following article is to discuss occupational health guidelines for the management of low back pain.
Occupational Health Guidelines for the Management of Low Back Pain: an International Comparison
Abstract
Background: The enormous socioeconomic burden of low back pain emphasizes the need to manage this problem, especially in an occupational context effectively. To address this, occupational guidelines have been issued in various countries.
Aims: To compare available international guidelines for managing low back pain in an occupational health care setting.
Methods: The guidelines were compared regarding generally accepted quality criteria using the AGREE instrument and also summarised regarding the guideline committee, the presentation, the target group, and assessment and management recommendations (that is, advice, return to work strategy, and treatment).
Results and Conclusions: The results show that the guidelines variously met the quality criteria. Common flaws concerned the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the extent to which editors and developers were independent. There was general agreement on numerous issues fundamental to occupational health management of back pain. The assessment recommendations included diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery. The guidelines also agreed on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most prevalent health issues treated in chiropractic offices. Although the following article describes low back pain as a self limiting condition, the cause of an individual’s LBP can also trigger debilitating and severe pain and discomfort of left untreated. It’s important for an individual with symptoms of low back pain to seek proper treatment with a chiropractor to properly diagnose and treat their health issues as well as prevent them from returning in the future. Patients who experience low back pain for more than 3 months are less than 3 percent likely to return to work. Chiropractic care is a safe and effective alternative treatment option which can help restore the original function of the spine. Furthermore, a doctor of chiropractic, or chiropractor, can provide lifestyle modifications, such as nutritional and fitness advice, to speed up the patient’s recovery process. Healing through movement is essential for LBP recovery.
Low back pain (LBP) is one of the industrial countries’ most common health problems. Despite its benign nature and sound course, LBP is commonly associated with incapacity, productivity loss due to sick leave, and high societal costs.[1]
Because of that impact, there is an obvious need for effective management strategies based on scientific evidence derived from studies of sound methodological quality. Usually, these are randomized controlled trials (RCTs) on the effectiveness of therapeutic interventions, diagnostic studies, or prospective observational studies on risk factors or side effects. The scientific evidence, summarised in systematic reviews and meta-analyses, provides a solid basis for guidelines on managing LBP. In a previous paper, Koes et al. compared various existing clinical guidelines for managing LBP targeted at primary healthcare professionals, showing a considerable commonality.[2]
The problems in occupational health care are different. Management focuses mainly on counseling the worker with LBP and addressing the issues of assisting them to continue working or return to work (RTW) after sick listing. However, LBP is also an important issue in occupational health care because of the associated incapacity for work, productivity loss, and sick leave. Several guidelines, or sections of guidelines, have now been published dealing with the specific issues of management in an occupational health care setting. Since the evidence is international, it would be expected that the recommendations of different occupational guidelines for LBP would be more or less similar. However, it is not clear whether the guidelines meet currently accepted quality criteria.
This paper critically appraises available occupational guidelines on managing LBP and compares their assessment and management recommendations.
Main Messages
In various countries, occupational health guidelines are issued to improve the management of low back pain in an occupational context.
Common flaws of these guidelines concern the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the independence of editors and developers.
In general, the assessment recommendations in the guidelines consisted of diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery.
There is general agreement on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Methods
Guidelines on the occupational health management of LBP were retrieved from the authors’ personal files. Retrieval was checked by a Medline search using the keywords low back pain, guidelines, and occupational up to October 2001, and personal communication with experts in the field. Policies had to meet the following inclusion criteria:
Guidelines aimed at managing workers with LBP (in occupational health care settings or addressing occupational issues) or separate sections of policies that dealt with these topics.
Guidelines are available in English or Dutch (or translated into these languages).
The exclusion criteria were:
Guidelines on primary prevention (that is, prevention before the onset of the symptoms) of work-related LBP (for example, lifting instructions for workers).
Clinical guidelines for the management of LBP in primary care.[2]
The quality of the included guidelines was appraised using the AGREE instrument, a generic tool designed primarily to help guideline developers and users assess the methodological quality of clinical practice guidelines.[3]
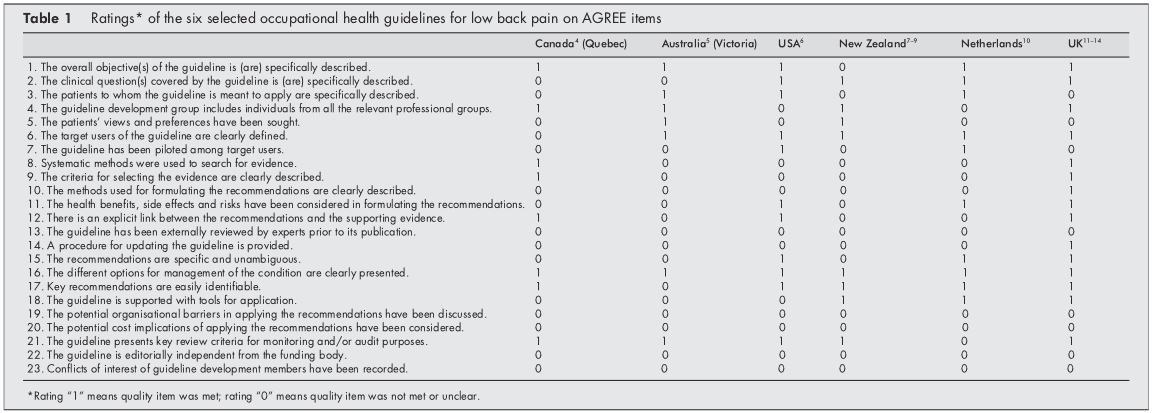
The AGREE instrument provides a framework for assessing the quality on 24 items (table 1), each rated on a four-point scale. The full operationalization is available on www.agreecollaboration.org.
Two reviewers (BS and HH) independently rated the quality of the guidelines and then met to discuss disagreements and to reach a consensus on the ratings. When they could not agree, a third reviewer (MvT) reconciled the remaining differences and decided on the ratings. To facilitate analysis in this review, ratings were transformed into dichotomous variables of whether each quality item was or was not met.
The assessment recommendations were summarised and compared to recommendations on advice, treatment, and return to work strategies. The selected guidelines were further characterized and reached regarding the guideline committee, the presentation of the procedure, the target group, and the extent to which the recommendations were based on available scientific evidence. All of this information was extracted directly from the published guidelines.
Policy Implications
The management of low back pain in occupational health care should follow evidence-based guidelines.
Future occupational guidelines for managing low back pain and updates of those guidelines should consider the criteria for proper development, implementation, and evaluation of approaches as suggested by the AGREE collaboration.
Results
Selection of Studies
Our search found ten guidelines, but four were excluded because they dealt with the management of LBP in primary care,[15] were aimed at the guidance of sick-listed employees in general (not specifically LBP),[16] were intended for the primary prevention of LBP at work,[17] or were not available in English or Dutch.[18] The final selection, therefore, consisted of the following six guidelines, listed by date of issue:
(1) Canada (Quebec). A scientific approach to the assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Quebec Canada (1987).[4]
(2) Australia (Victoria). Guidelines for the management of employees with compensable low back pain. Victorian WorkCover Authority, Australia (1996).[5] (This is a revised version of guidelines developed by the South Australian WorkCover Corporation in October 1993.)
(3) the USA. Occupational Medicine Practice Guidelines. American College of Occupational and Environmental Medicine. USA (1997).[6]
(4) New Zealand
(a)Active and working! Managing acute low back pain in the workplace. Accident Compensation Corporation and National Health Committee. New Zealand (2000).[7]
(b)Patient guide to acute low back pain management. Accident Compensation Corporation and National Health Committee. New Zealand (1998).[8]
(c) Assess psychosocial yellow flags in acute low back pain. Accident Compensation Corporation and National Health Committee. New Zealand (1997).[9]
(5) the Netherlands. Dutch guideline for managing occupational physicians of employees with low back pain. Dutch Association of Occupational Medicine (NVAB). Netherlands (1999).[10]
(6) the UK
(a)Occupational health guidelines for managing low back pain at work principal recommendations. Faculty of Occupational Medicine. UK (2000).[11]
(b)Occupational health guidelines for managing low back pain at work leaflet for practitioners. Faculty of Occupational Medicine. UK (2000).[12]
(c)Occupational health guidelines for managing low back pain at work evidence review. Faculty of Occupational Medicine. UK (2000).[13]
(d)The Back Book, The Stationery Office. UK (1996).[14]
Two guidelines (4 and 6) could not be evaluated independently from additional documents to which they refer (4bc, 6bd), so these documents were also included in the review.
Appraisal of the Quality of the Guidelines
Initially, there was an agreement between the two reviewers regarding 106 (77%) of the 138 item ratings. After two meetings, the consensus was reached for all but four items, which required adjudication by the third reviewer. Table 1 presents the final ratings.
All included guidelines presented the different options for managing LBP in occupational health. In five of the six policies, the overall objectives of the procedure were explicitly described,[46, 1014] the target users of the system were clearly defined,[514] easily identifiable key recommendations were included,[4, 614] or critical review criteria were presented for monitoring and audit purposes.[49, 1114]
The results of the AGREE appraisal showed that none of the guidelines paid sufficient attention to potential organizational barriers and cost implications in implementing the recommendations. It was also unclear for all included guidelines whether or not they were editorially independent of the funding body and whether or not there were conflicts of interest for the members of the guideline development committees. Furthermore, it was unclear for all guidelines whether experts had externally reviewed the policies before publication. Only the UK guideline clearly described the method used to formulate the recommendations and provided for updating the approach.[11]
Development of the Guidelines
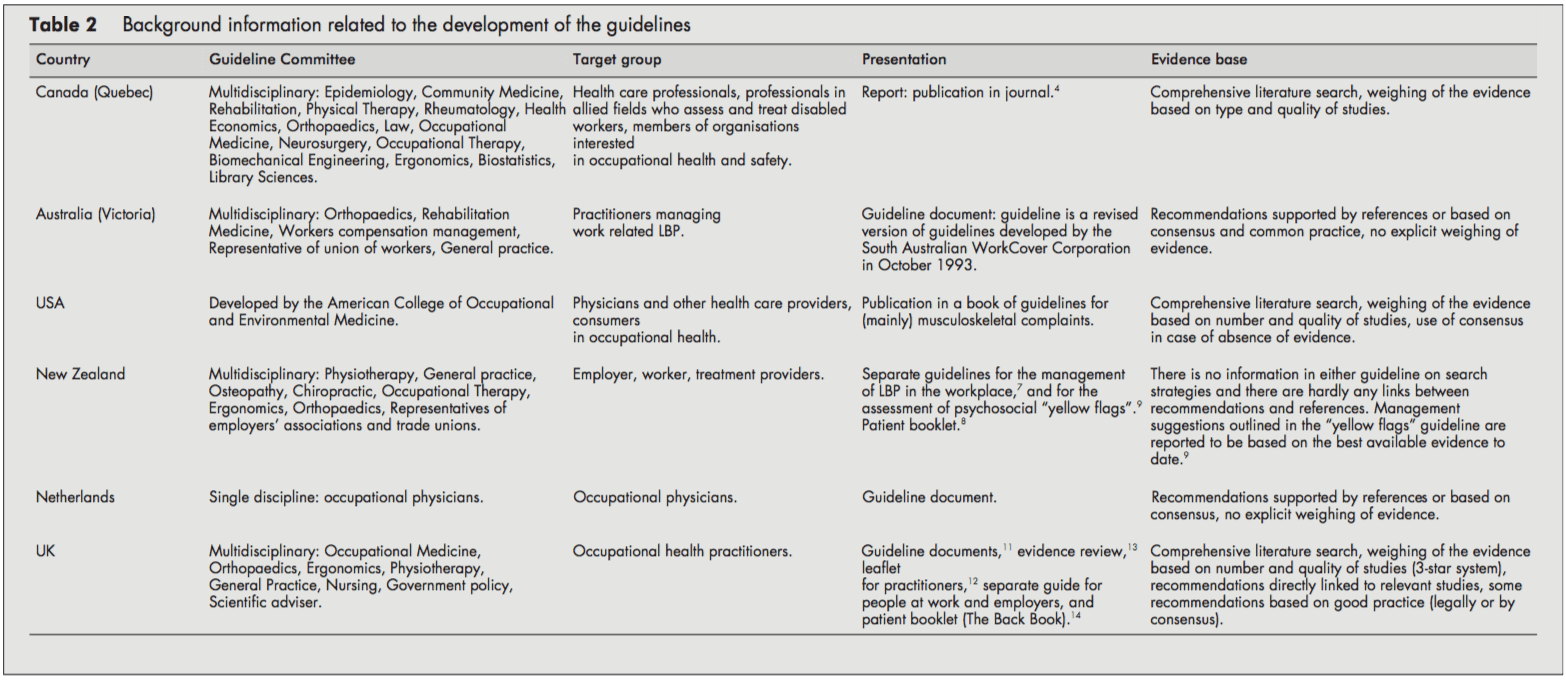
Table 2 presents background information on the development process of the guidelines.
The target users for the guidelines were physicians and other healthcare providers in the field of occupational healthcare. Several policies were also directed at informing employers, workers [68, 11, 14], or members of organizations interested in occupational health.[4] The Dutch guideline was only targeted at the occupational health physician.[10]
The guideline committees responsible for developing the guidelines were generally multidisciplinary, including disciplines like epidemiology, ergonomics, physiotherapy, general practice, occupational medicine, occupational therapy, orthopedics, and representatives of employers’ associations and trade unions. Chiropractic and osteopathic representatives were in the guideline committee of the New Zealand guidelines.[79] The Quebec task force (Canada) also included representatives of rehabilitation medicine, rheumatology, health economics, law, neurosurgery, biomechanical engineering, and library sciences. In contrast, the guideline committee of the Dutch guideline consisted only of occupational physicians.[10]
The guidelines were issued as a separate document,[4, 5, 10] as a chapter in a textbook,[6] or as several interrelated documents.[79, 1114]
The UK,[13] the USA,[6] and Canadian[4] guidelines provided information on the search strategy applied to the identification of relevant literature and the weighing of the evidence. On the other hand, the Dutch[10] and the Australian[5] guidelines supported their recommendations only by references. The New Zealand guidelines showed no direct links between suggestions and concerns [79]. The reader was referred to other literature for background information.
Patient Population and Diagnostic Recommendations
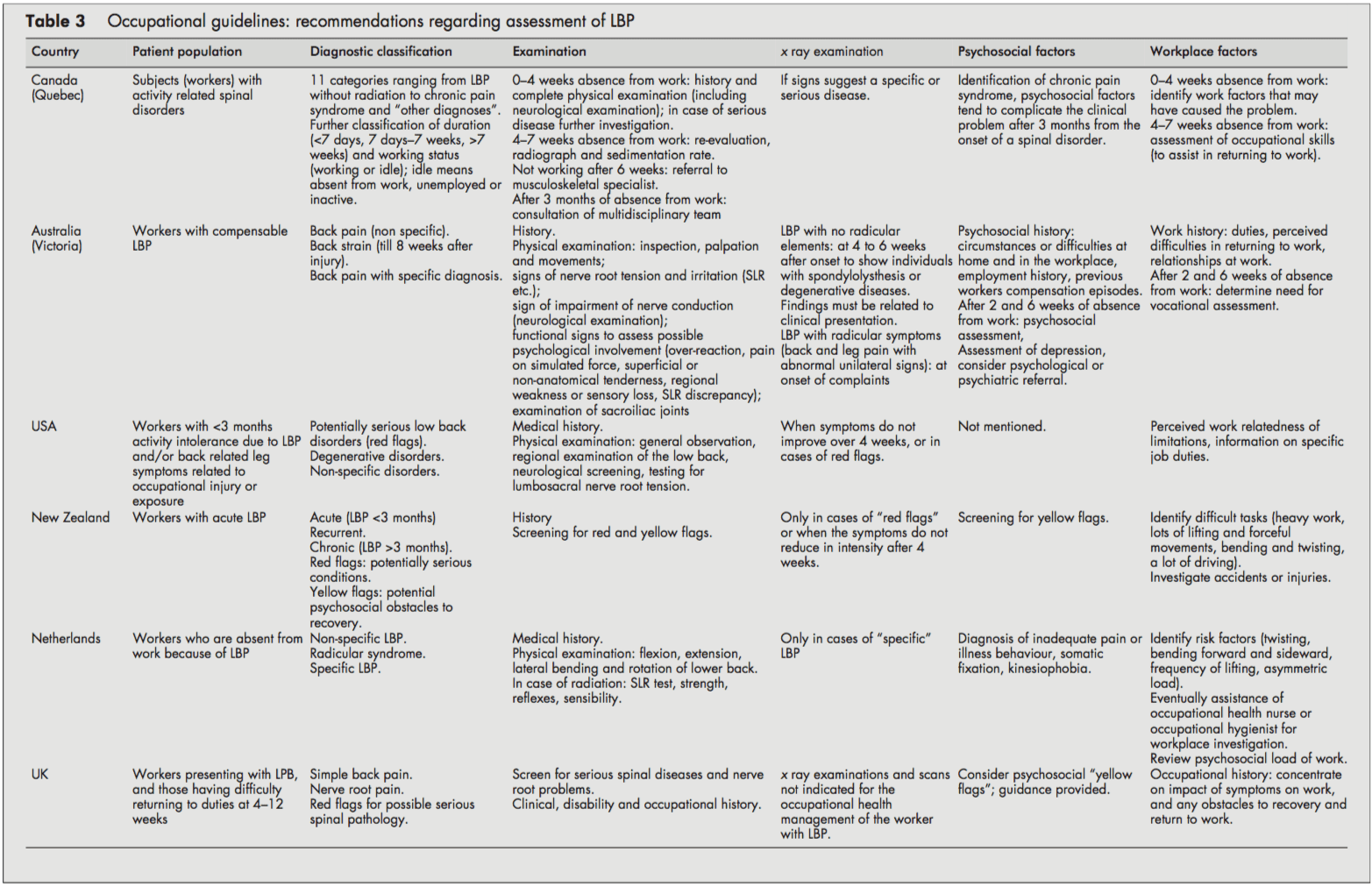
Although all guidelines focused on workers with LBP, it was often unclear whether they dealt with acute or chronic LBP or both. Acute and chronic LBP were often not defined, and cut-off points were given (for example, <3 months). It was usually unclear whether these referred to the onset of symptoms or absence from work. However, the Canadian guideline introduced a classification system (acute/subacute/ chronic) based on the distribution of claims of spinal disorders by time since absence from work.[4]
All guidelines distinguished specific and non-specific LBP. Specific LBP concerns the potentially serious red flag conditions like fractures, tumors, or infections, and the Dutch and UK guidelines also distinguish the radicular syndrome or nerve root pain.[1013] All procedures were consistent in their recommendations to take a clinical history and to carry out a physical examination, including neurological screening. In cases of suspected specific pathology (red flags), x-ray examinations were recommended by most guidelines. In addition, New Zealand and the US guideline also recommended an x-ray examination when symptoms did not improve after four weeks.[6, 9] The UK guideline stated that x-ray examinations are not indicated and do not assist occupational health management of the patient with LBP (distinct from any clinical indications).[1113]
Most guidelines considered psychosocial factors as yellow flags as obstacles to recovery that healthcare providers should address. The New Zealand[9] and UK guidelines [11, 12] explicitly listed factors and suggested questions to identify those psychosocial yellow flags.
All guidelines addressed the importance of the clinical history identifying physical and psychosocial workplace factors relevant to LBP, including physical demands of work (manual handling, lifting, bending, twisting, and exposure to whole-body vibration), accidents or injuries, and perceived difficulties in returning to work or relationships at work. The Dutch and the Canadian guidelines contained recommendations to carry out a workplace investigation[10] or an assessment of occupational skills when necessary.[4]
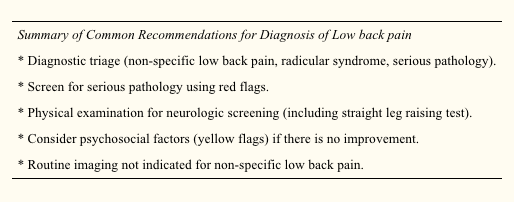
Summary of Recommendations for the Assessment of LBP
Diagnostic triage (non-specific LBP, radicular syndrome, specific LBP).
Exclude red flags and neurological screening.
Identify psychosocial factors and potential obstacles to recovery.
Identify workplace factors (physical and psychosocial) that may be related to the LBP problem and return to work.
X-Ray examinations are restricted to suspected cases of specific pathology.
Recommendations Regarding Information and Advice, Treatment, and Return to Work Strategies
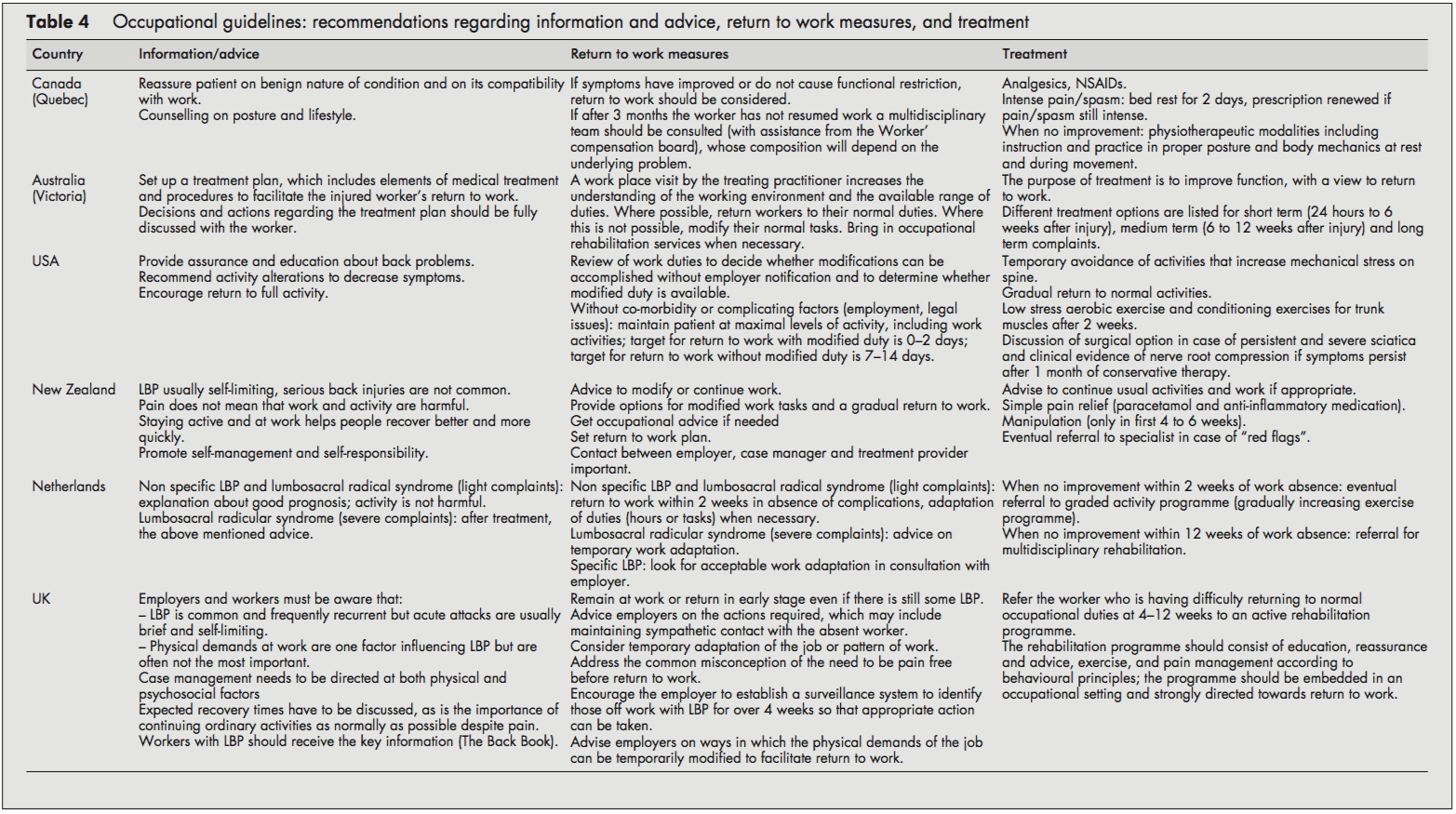
Most guidelines recommended reassuring the employee and providing information about LBP’s self-limiting nature and good prognosis. Encouragement of return to ordinary activity as generally as possible was frequently advised.
In line with the recommendation to return to regular activity, all guidelines also stressed the importance of returning to work as rapidly as possible, even if there is still some LBP and, if necessary, starting with modified duties in more severe cases. Work duties could then be increased gradually (hours and tasks) until total return to work was reached. The US and Dutch guidelines provided detailed time schedules for return to work. The Dutch approach proposed a return to work within two weeks with an adaptation of duties when necessary.[10] The Dutch system also stressed the importance of time-contingent management about a return to work.[10] The US guideline proposed every attempt to maintain the patient at maximal levels of activity, including work activities; targets for disability duration in terms of return to work were given as 02 days with modified duties and 714 days if modified duties are not used/available.[6] In contrast to the others, the Canadian guideline advised return to work only when symptoms and functional restrictions had improved.[4]
The most frequently recommended treatment options in all the included guidelines were: medication for pain relief,[5, 7, 8] gradually progressive exercise programs,[6, 10] and multidisciplinary rehabilitation.[1013] The US guideline recommended referral within two weeks to an exercise program consisting of aerobic exercises, conditioning exercises for trunk muscles, and exercise quota.[6] The Dutch guideline recommended that if there is no progress within two weeks of work absence, workers should be referred to a graded activity program (gradually increasing exercises) and, if there is no improvement by four weeks, to a multidisciplinary rehabilitation program.[10] The UK guideline recommended that workers who have difficulty returning to regular occupational duties by 412 weeks should be referred to an active rehabilitation program. This rehabilitation program should include education, reassurance and advice, a progressive vigorous exercise and fitness program, and pain management according to behavioral principles; it should be embedded in an occupational setting and directed firmly toward a return to work.[11-13] Extensive lists of possible treatment options were presented in the guidelines of Canada and Australia [4, 5], although most of these were not based on scientific evidence.
Summary of Recommendations Regarding Information, Advice, Return to Work Measures, and Treatment in Workers with LBP
Reassure the worker and provide adequate information about LBP’s self-limiting nature and good prognosis.
Advise the worker to continue ordinary activities or to return to regular exercise and work as soon as possible, even if there is still some pain.
Most workers with LBP return to more or less regular duties quite rapidly. Consider temporary adaptations of work duties (hours/tasks) only when necessary.
When a worker fails to return to work within 212 weeks (there is considerable variation in the time scale in different guidelines), refer them to a gradually increasing exercise program, or multidisciplinary rehabilitation (exercises, education, reassurance, and pain management following behavioral principles). These rehabilitation programs should be embedded in an occupational setting.
Discussion
The management of LBP in an occupational health setting must address the relation between low back complaints and work and develop strategies aimed at a safe return to work. This review compared available occupational health guidelines from various countries. Policies are rarely indexed in Medline, so when searching for guidelines, we had to rely primarily on personal files and personal communication.
Quality Aspects and Development Process of the Guidelines
The assessment by the AGREE instrument[3] showed some differences in the quality of the guidelines reviewed, which may partly reflect the variation in the dates of development and publication of the guidelines. The Canadian guideline, for example, was published in 1987 and the Australian guideline in 1996.[4, 5] The other guidelines were more recent and incorporated a more extensive evidence base and more up to date guideline methodology.
Several common flaws related to the development process of the guidelines were shown by the assessment by the AGREE instrument. Firstly, it is important to make clear whether a guideline is editorially independent from the funding body, and whether there are conflicts of interest for the members of the guideline committee. None of the included guidelines clearly reported these issues. Further, reported external review of the guideline by clinical and methodological experts prior to publication was also lacking in all guidelines included in this review.
Several guidelines provided comprehensive information on the way relevant literature was searched and translated into recommendations.[4, 6, 11, 13] Other guidelines supported their recommendations by references,[5, 7, 9, 10] but this does not permit assessment of the robustness of the guidelines or their recommendations.
Guidelines depend on the scientific evidence, which changes over time, and it is striking that only one guideline provided for future update.[11, 12] Possibly there are updates planned for the other guidelines but they are not explicitly stated (and conversely stating there will be future update does not mean it will actually occur). This lack of reporting may also hold true for other AGREE criteria that we rated negatively. The use of the AGREE framework as a guide for both the development and the reporting of guidelines should help to improve the quality of future guidelines.
Assessment and Management of LBP
The diagnostic procedures recommended in the occupational health guidelines were largely similar to the recommendations of clinical guidelines,[2] and, logically, the main difference was the emphasis on addressing occupational issues. The reported methods for addressing workplace factors in the assessment of LBP of the individual worker concerned the identification of difficult tasks, risk factors, and obstacles for return to work by occupational histories. Obviously, these obstacles for return to work not only concern physical load factors, but also work related psychosocial problems regarding responsibilities, cooperation with co-workers, and the social atmosphere at the workplace.[10] Screening for work related psychosocial yellow flags may help to identify those workers who are at risk for chronic pain and disability.[1113]
A potentially important feature of the guidelines is that they were consistent regarding their recommendations to reassure the employee with LBP, and to encourage and support return to work even with some persisting symptoms. There is general consensus that most workers do not have to wait until they are completely free of pain before returning to work. The lists of treatment options provided by the Canadian and Australian guidelines may reflect the lack of evidence at that time,[4, 5] leaving users of the guidelines to choose for themselves. It is, however, questionable whether such lists really contribute to improved care, and in our view guideline recommendations should be based on sound scientific evidence.
The US, Dutch, and UK occupational guidelines[6, 1013] recommend that active multidisciplinary treatment is the most promising intervention for return to work, and this is supported by strong evidence from RCTs.[19, 20] However, more research is still needed to identify the optimum content and intensity of those treatment packages.[13, 21]
Despite some evidence for a contribution of workplace factors in the aetiology of LBP,[22] systematic approaches for workplace adaptations are lacking, and are not offered as recommendations in the guidelines. Perhaps this represents a lack of confidence in the evidence on the overall impact of workplace factors, a difficulty of translation into practical guidance, or because these issues are confounded with local legislation (which was hinted at in the UK guideline[11]). It may be that the participatory ergonomics intervention, which proposes consultations with the worker, the employer, and an ergonomist, will turn out to be a useful return to work intervention.[23, 24] The potential value of getting all the players onside[25] was stressed in the Dutch and the UK guidelines,[1113] but further evaluation of this approach and its implementation is required.
Development of Future Guidelines in Occupational Health Care
The purpose of this review was to give both an overview and a critical appraisal of occupational guidelines for the management of LBP. The critical appraisal of the guidelines is meant to help direct future development and planned updates of guide- lines. In the still emerging field of guideline methodology we consider all past initiatives as laudable; we recognise the need for clinical guidance, and appreciate that guidelines developers cannot wait for research to provide all the methodology and evidence required. However, there is room for improvement and future guidelines and updates should consider the criteria for proper development, implementation, and evaluation of guidelines as suggested by the AGREE collaboration.
The implementation of the guidelines is beyond the scope of this review, but it was noted that none of the guideline documents specifically described implementation strategies, so it is uncertain to what extent the target groups may have been reached, and what effects that may have had. This may be a fruitful area for further research.
The very existence of these occupational health guidelines shows that existing primary care clinical guidelines for LBP2 are considered inappropriate or insufficient for occupational health care. There is a clear perception internationally that the needs of the worker experiencing back pain are intrinsically linked to a variety of occupational issues not covered by usual primary care guidance and, consequently, practice. What emerges is that, despite the methodological flaws, considerable agreement is evident on a range of fundamental occupational health strategies for managing the worker with back pain, some of which are innovative and challenge previously held views. There is agreement on the fundamental message that prolonged work loss is detrimental, and that early work return should be encouraged and facilitated; there is no need to wait for complete symptom resolution. Although the recommended strategies vary somewhat, there is considerable agreement on the value of positive reassurance and advice, availability of (temporary) modified work, addressing workplace factors (getting all the players onside), and rehabilitation for workers having difficulty returning to work.
Acknowledgements
This study was supported by the Dutch Health Care Insurance Council (CVZ), grant DPZ no. 169/0, Amstelveen, Netherlands. J B Staal is currently working at the Department of Epidemiology, Maastricht University, PO Box 616 6200 MD Maastricht, Netherlands. W van Mechelen is also part of the Research Centre on Physical Activity, Work and Health, Body@work TNO-VUmc.
In conclusion, symptoms of low back pain are one of the most common health issues associated with work injuries. Because of it, several occupational health guidelines have been established for the management of low back pain. Chiropractic care, among other treatment methods, may be utilized in order to help the patient find relief from their LBP. Furthermore, the article above demonstrated the safety and effectiveness of a variety of traditional as well as alternative treatment options in the diagnosis, treatment and prevention of a variety of low back pain cases. However, further research studies are required in order to properly determine the efficiency of each individual treatment method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
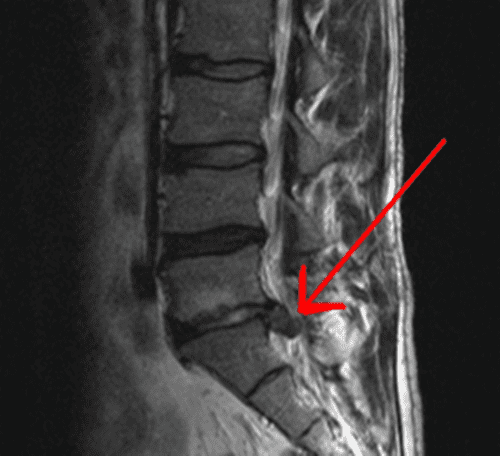
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Van Tulder MW, Koes BW, Bouter LM. A cost-of-illness study of back pain in the Netherlands. Pain 1995;62:233�40.
2. Koes BW, van Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international
comparison. Spine 2001;26:2504�14.
3. The AGREE Collaboration. Appraisal of Guidelines Research &
Evaluation Instrument, www.agreecollaboration.org.
4. Spitzer WO, Leblanc FE, Dupuis M. Scientific approach to the
assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine 1987;12(suppl 7S):1�59.
5. Victorian WorkCover Authority. Guidelines for the management of employees with compensable low back pain. Melbourne: Victorian WorkCover Authority, 1996.
6. Harris JS. Occupational medicine practice guidelines. Beverly, MA: OEM Press, 1997.
7. Accident Compensation Corporation and National Health Committee. Active and working! Managing acute low back pain in the workplace. Wellington, New Zealand, 2000.
8. Accident Compensation Corporation and National Health Committee, Ministry of Health. Patient guide to acute low back pain management. Wellington, New Zealand, 1998.
9. Kendall, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain. Risk factors for long-term disability and work loss. Wellington, New Zealand, Accident Rehabilitation & Compensation Insurance Corporation of New Zealand and the National Health Committee, 1997.
10. Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (Dutch Association of Occupational Medicine, NVAB). Handelen van de bedrijfsarts bij werknemers met lage-rugklachten. Richtlijnen voor Bedrijfsartsen. [Dutch guideline for the management of occupational physicians of employees with low back pain]. April 1999.
11. Carter JT, Birell LN. Occupational health guidelines for the management of low back pain at work�principal recommendations. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
12. Occupational health guidelines for the management of low back pain at work�leaflet for practitioners. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
13. Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work�evidence review. Occup Med 2001;51:124�35.
14. Roland M, et al. The back book. Norwich: The Stationery Office, 1996.
15. ICSI. Health care guideline. Adult low back pain. Institute for Clinical Systems Integration, 1998 (www.icsi.org/guide/).
16. Kazimirski JC. CMA policy summary: The physician�s role in helping patients return to work after an illness or injury. CMAJ 1997;156:680A�680C.
17. Yamamoto S. Guidelines on worksite prevention of low back pain. Labour standards bureau notification, No. 57. Industrial Health 1997;35:143�72.
18. INSERM. Les Lombalgies en milieu professionel: quel facteurs de risque et quelle prevention? [Low back pain at the workplace: risk factors and prevention]. Paris: les editions INSERM, Synthese bibliographique realise a la demande de la CANAM, 2000.
19. Lindstro?m I, Ohlund C, Eek C, et al. The effect of graded activity on patients with subacute low back pain: a randomised prospective clinical study with an operant-conditioning behavioural approach. Physical Therapy 1992;72:279�93.
20. Karjalainen K, Malmivaara A, van Tulder M, et al. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2001;26:262�9.
21. Staal JB, Hlobil H, van Tulder MW, et al. Return-to-work interventions for low back pain: a descriptive review of contents and concepts of working mechanisms. Sports Med 2002;32:251�67.
22. Hoogendoorn WE, van Poppel MN, Bongers PM, et al. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health 1999;25:387�403.
23. Loisel P, Gosselin L, Durand P, et al. A population-based, randomised clinical trial on back pain management. Spine 1997;22:2911�18.
24. Loisel P, Gosselin L, Durand P, et al. Implementation of a participatory ergonomics program in the rehabilitation of workers suffering from subacute back pain. Appl Ergon 2001;32:53�60.
25. Frank J, Sinclair S, Hogg-Johnson S, et al. Preventing disability from work-related low-back pain. New evidence gives new hope�if we can just get all the players onside. CMAJ 1998;158:1625�31.
According to the American Chiropractic Association, approximately 31 million people in the United States experience low back pain throughout their lifetime. Low back pain can occur due to a variety of injuries and/or conditions and it can range in severity. Trauma from an injury or an aggravated condition can cause symptoms ranging from mild and annoying to intense and debilitating. The most common type of low back pain is described as a dull, achy, burning or spasming sensation.
Diagnosing the source of a patient’s low back pain can be challenging, however, several healthcare professionals are qualified and experienced in the treatment of spinal health issues, including chiropractors and physical therapists. As a matter of fact, new guidelines from the American Medical Association, or the AMA, have suggested that people affected with low back pain should seek chiropractic care before seeking treatment from conventional medical doctors because chiropractors primarily focus on the diagnosis, treatment and prevention of injuries and/or conditions affecting the musculoskeletal and nervous system.
Chiropractic care is a well-known alternative treatment option commonly utilized to treat injuries and/or conditions causing low back pain. Regular chiropractic care can provide safe and effective, non-invasive treatment without the need to utilize drugs and/or medications. A chiropractor, or doctor of chiropractic, will commonly use spinal adjustments and manual manipulations to carefully correct any spinal misalignment, or subluxation, along the lumbar spine which may be causing symptoms of low back pain. Other treatment methods commonly utilized in chiropractic care include, hot or cold compresses, massage and physical therapy modalities like interferential therapy or transcutaneous electrical nerve stimulations, or TENS and spinal decompression therapy. A chiropractor may also offer nutritional advice and fitness plans to speed up the patient’s recovery process.
By restoring the original alignment of the spine, a chiropractor can help improve the function of the spine by reducing pain and discomfort, decreasing inflammation, and improving range of motion and flexibility as well as increasing strength. Chiropractic care allows the human body to naturally heal itself in order to better be able to manage symptoms associated with low back pain. Based on the diagnosis of a patient, a doctor of chiropractic may also refer patients to other healthcare professionals for further treatment. The purpose of the following article is to demonstrate an overview of updated clinical treatment guidelines for the proper management of non-specific low back pain in a primary care setting.
An Updated Overview of Clinical Guidelines for the Management of Non-Specific Low Back Pain in Primary Care
Abstract
The aim of this study was to present and compare the content of (inter)national clinical guidelines for the management of low back pain. To rationalise the management of low back pain, evidence-based clinical guidelines have been issued in many countries. Given that the available scientific evidence is the same, irrespective of the country, one would expect these guidelines to include more or less similar recommendations regarding diagnosis and treatment. We updated a previous review that included clinical guidelines published up to and including the year 2000. Guidelines were included that met the following criteria: the target group consisted mainly of primary health care professionals, and the guideline was published in English, German, Finnish, Spanish, Norwegian, or Dutch. Only one guideline per country was included: the one most recently published. This updated review includes national clinical guidelines from 13 countries and 2 international clinical guidelines from Europe published from 2000 until 2008. The content of the guidelines appeared to be quite similar regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features for acute low back pain were the early and gradual activation of patients, the discouragement of prescribed bed rest and the recognition of psychosocial factors as risk factors for chronicity. For chronic low back pain, consistent features included supervised exercises, cognitive behavioural therapy and multidisciplinary treatment. However, there are some discrepancies for recommendations regarding spinal manipulation and drug treatment for acute and chronic low back pain. The comparison of international clinical guidelines for the management of low back pain showed that diagnostic and therapeutic recommendations are generally similar. There are also some differences which may be due to a lack of strong evidence regarding these topics or due to differences in local health care systems. The implementation of these clinical guidelines remains a challenge for clinical practice and research.
Keywords:Low back pain, Clinical guidelines, Review, Diagnosis, Treatment
Dr. Alex Jimenez’s Insight
Low back pain is one of the most common reasons for doctor office visits each year. In fact, about 80 percent of the population in the United States will suffer from back pain at least once throughout their lifetime. Regular chiropractic care can help prevent, treat and manage low back pain symptoms. Chiropractic care can provide many other benefits as well. Patient’s who have received chiropractic care for injuries and/or conditions affecting the musculoskeletal and nervous systems have experienced improvements to their digestive health and have reported better and deeper sleep after a visit to a chiropractor office. Furthermore, research studies have demonstrated that chiropractic care can help build your immune system. Chiropractic care has even been associated with stress management, reducing depression and anxiety levels. Chiropractic care can provide low back pain relief and improve overall health and wellness.
Introduction
Low back pain remains a condition with a relatively high incidence and prevalence. Following a new episode, the pain typically improves substantially but does not resolve completely during the first 4�6 weeks. In most people the pain and associated disability persist for months; however, only a small proportion remains severely disabled [1]. For those whose pain does resolve completely, recurrence during the next 12 months is not uncommon [2, 3].
There is a wide acceptance that the management of low back pain should begin in primary care. The challenge for primary care clinicians is that back pain is but one of many conditions that they manage. For example while back pain, in absolute numbers, is the eighth most common condition managed by Australian GPs, it only accounts for 1.8% of their case load [4]. To assist primary care practitioners to provide care that is aligned with the best evidence, clinical practice guidelines have been produced in many countries around the world.
The first low back pain guideline was published in 1987 by the Quebec Task Force with authors pointing to the absence of high-quality evidence to guide decision making [5]. Since that time there has been a strong growth in research addressing diagnosis and prognosis but especially research on therapy. As an example of this growth, at the time of the Spitzer guideline [5] there were only 108 randomised controlled trials evaluating physiotherapy treatments for low back pain but as at April 2009 there were 958.1 The Cochrane database (Central) currently lists more than 2500 controlled trials evaluating treatment for back and neck pain. The evidence from these trials for most interventions is summarised in systematic reviews and meta-analysis. The Cochrane Back Review Group, for example, has now published 32 systematic reviews of randomised controlled trials evaluating interventions for low back pain. In the near future, systematic reviews of studies evaluating diagnostic intervention for low back pain will also be included in the Cochrane Library.
This dramatic growth in research would be a comfort to those who were members of the original Quebec Task Force but perhaps a challenge to those who served on committees for later guidelines. With a large and ever increasing research base to inform guidelines two potential problems arise. The first and most obvious is that the recommendations in the guidelines may become out of date. The second is that with a wealth of information to consider, the various committees producing guidelines may produce quite different treatment recommendations. At the same time one can argue that if more precise and valid information becomes available recommendations will become more similar. A previous systematic review of clinical practice guidelines was conducted in 2001 [6]. In that review we assessed the available clinical guidelines from 11 countries and concluded that the guidelines provided generally similar recommendations regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features were the early and gradual activation of patients, the discouragement of prescribed bed rest, and the recognition of psychosocial factors as risk factors for chronicity. However, there were discrepancies for recommendations regarding exercise therapy, spinal manipulation, muscle relaxants, and patient information.
Bouwmeester et al. [7] concluded recently that the quality of mono- and multidisciplinary clinical guidelines for the management of low back pain, as measured with the AGREE instrument has improved over time. The present article focuses on the actual content of national clinical guidelines on low back pain which have been issued since 2001. These guidelines are compared regarding the content of their recommendations, the target group, the guideline committee and its procedures, and the extent to which the recommendations were based on the available literature (the scientific evidence). We also highlight any changes in recommendations that have occurred over time in comparison with our previous review [6].
Methods
Clinical guidelines were searched using electronic databases covering the period 2000�2008: Medline (key words: low back pain, clinical guidelines), PEDro (key words: low back pain, practice guidelines, combined with AND), National Guideline Clearinghouse (www.guideline.gov; key word: low back pain), and National Institute for Health and Clinical Excellence (NICE) (www.nice.org.uk; key word: low back pain). Guidelines used in the previous review were checked for updates. We also checked the content and reference list of relevant reviews on guidelines, included a search on the Web of Science citation index for articles citing the previous review and asked experts in the field. To be included in this review, the guidelines had to meet the following criteria: (1) the guideline concerned the diagnosis and clinical management of low back pain, (2) the guideline was targeted at a multidisciplinary audience in the primary care setting, and (3) the guideline was available in English, German, Finnish, Spanish, Norwegian or Dutch because documents in these languages could be read by the reviewers. Only one guideline was included per country unless there were separate guidelines for acute and chronic low back pain. Where more than one eligible guideline was available for a country, we included the most recent guideline issued by a national body. Guidelines from the following countries/regions and agencies (year of publication) were included:
Australia, National Health and Medical Research Council (2003) [8];
Austria, Center for Excellence for Orthopaedic Pain Management Speising (2007) [9];
Canada, Clinic on Low back Pain in Interdisciplinary Practice (2007) [10];
Europe, COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care (2004) [11];
Europe, COST B13 Working Group on Guidelines for the Management of Chronic Low Back Pain in Primary Care (2004) [12];
Finland, Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis Fenniae. Duodecim (2008) [13];
France, Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) [14];
Germany, Drug Committee of the German Medical Society (2007) [15];
Italy, Italian Scientific Spine Institute (2006) [16];
New Zealand, New Zealand Guidelines Group (2004) [17];
Norway, Formi & Sosial- og helsedirectorated (2007) [18];
Spain, the Spanish Back Pain Research Network (2005) [19];
The Netherlands, The Dutch Institute for Healthcare Improvement (CBO) (2003) [20];
United Kingdom, National Health Service (2008) [21]; and
United States, American College of Physicians and the American Pain Society (2007) [22].
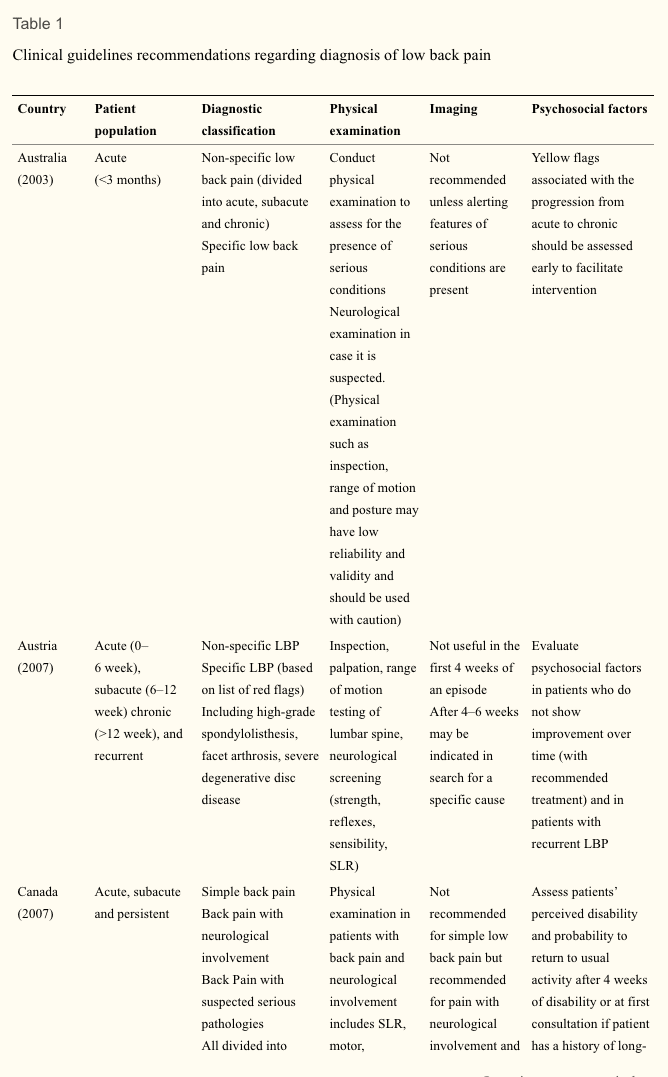
Data regarding the diagnostic and therapeutic recommendations as well as background information of the guideline process were extracted from the guidelines by four of the authors, each assessing 3�4 guidelines. The Finnish and Norwegian guidelines were assessed by colleagues with relevant language skills from The Netherlands and Finland. The focus was on the process of guideline development and the recommendations for diagnosis and treatment. We used the same data categories as in the previous review to facilitate comparisons (see Tables 1, ?,2,2, ?,33).
Results
Patient Population
Each of the guidelines considered the duration of symptoms but they vary in their scope and definitions. For example, the guidelines from Australia and New Zealand focus on acute low back pain whereas the guidelines from Austria and Germany consider acute, subacute, chronic and recurrent low back pain. The cut-off for chronic is not always specified but when it was, 12 weeks was used. Sometimes the word persistent rather than chronic was used. Two guidelines (Austrian and German) provide recommendations for recurrent low back pain but do not explicitly define �recurrent�.
Diagnostic Recommendations
Table 1 compares the diagnostic classification and the recommendations on diagnostic procedures in the various guidelines. All guidelines recommend a diagnostic triage where patients are classified as having (2) non-specific low back pain, (2) suspected or confirmed serious pathology (�red flag� conditions such as tumour, infection or fracture) and (3) radicular syndrome. Some guidelines, e.g. the Australian and New Zealand guidelines, do not distinguish between non-specific low back pain and radicular syndrome. The German guideline also classifies a group of patients who are at risk for chronicity, based on �yellow flags�.
All guidelines are consistent in their recommendations that diagnostic procedures should focus on the identification of red flags and the exclusion of specific diseases (sometimes including radicular syndrome). Red flags include, for example, age at onset (<20 or >55 years), significant trauma, unexplained weight loss and widespread neurologic changes. The types of physical examination and physical tests that are recommended show some variation. Some, such as the European guideline, limit the examination to a neurological screen whereas others advocate a more comprehensive musculoskeletal (including inspection, range of motion/spinal mobility, palpation, and functional limitation) and neurological examination. The components of the neurologic screening are not always explicit but where they are, comprise testing of strength, reflexes, sensation and straight leg raising.
None of the guidelines recommend routine use of imaging, with imaging recommended at the initial visit only for cases of suspected serious pathology (e.g. Australian, European) or where the proposed treatment (e.g. manipulation) requires the exclusion of a specific cause of low back pain (French). Imaging is sometimes recommended where sufficient progress is not being made but the time cut-off varies from 4 to 7 weeks. Guidelines often recommend MRI in cases with red flags (e.g. European, Finland, Germany).
All guidelines mention psychosocial factors associated with poor prognosis with some describing them as �yellow flags�. There is, however, considerable variation in the amount of details given about how to assess �yellow flags� or the optimal timing of the assessment. The Canadian and the New Zealand guidelines provide specific tools for identifying yellow flags and clear guidelines for what should be done once yellow flags are identified.
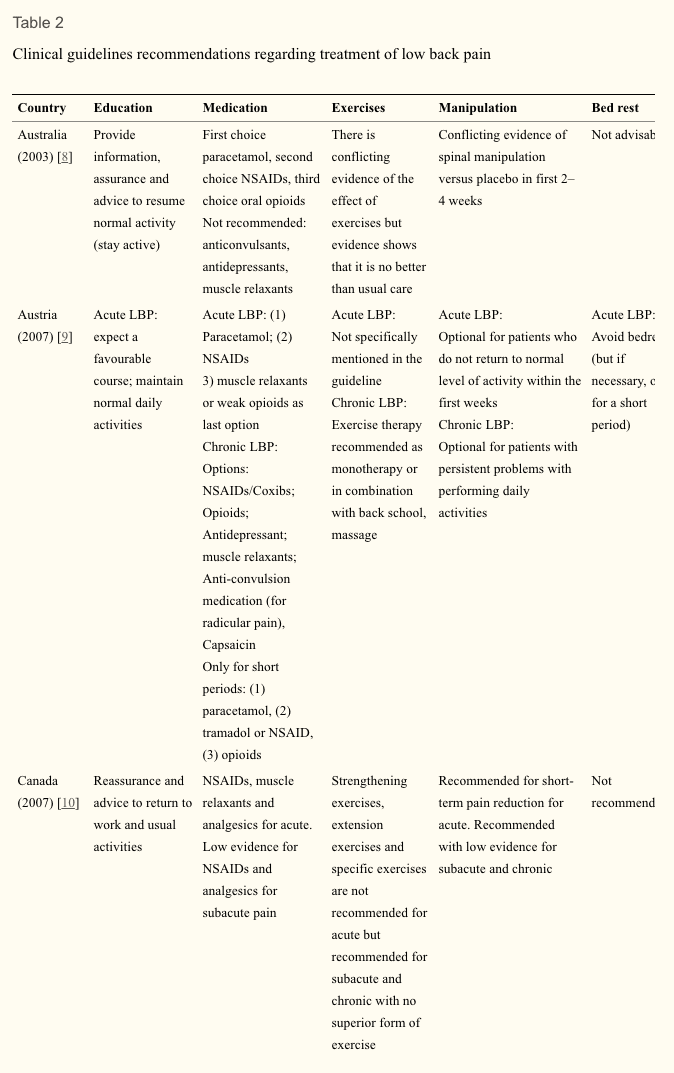
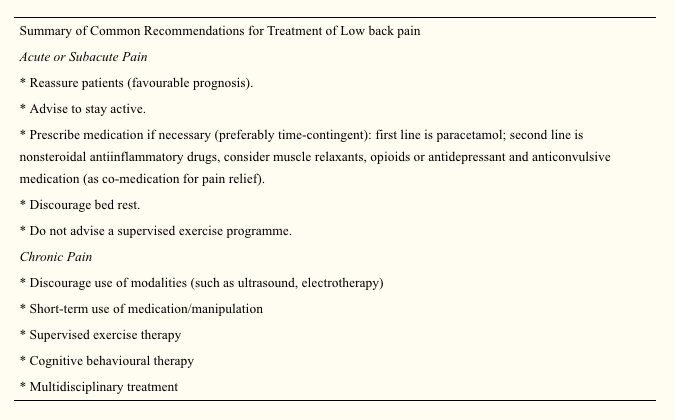
Therapeutic Recommendations
Table 2 compares therapeutic recommendations given in the various guidelines. Patient advice and information is recommended in all guidelines. The common message is that patients should be reassured that they do not have a serious disease, that they should stay as active as possible and progressively increase their activity levels. Compared with the previous review, the current guidelines increasingly mention early return to work (despite having low back pain) in their list of recommendations.
Recommendations for the prescription of medication are generally consistent. Paracetamol/acetaminophen is usually recommended as a first choice because of the lower incidence of gastrointestinal side effects. Nonsteroidal anti-inflammatory drugs are the second choice in cases where paracetamol is not sufficient. There is some variation between guidelines with regard to recommendations for opioids, muscle relaxants, steroids, antidepressant and anticonvulsive medication as co-medication for pain relief. Where the mode of consumption of analgesics is described, time-contingent rather than pain-contingent use, is advocated.
There is now broad consensus that bed rest should be discouraged as a treatment for low back pain. Some guidelines state that if bed rest is indicated because of severity of pain, then it should not be advised for more than 2 days (e.g., Germany, New Zealand, Spain, Norway). The Italian guideline advises 2�4 days of bed rest for major sciatica but does clearly describe how major sciatica differs from sciatica where bed rest is contraindicated.
There is also consensus that a supervised exercise programme (as distinct from encouraging resumption of normal activity) is not indicated for acute low back pain. Those guidelines that consider subacute and chronic low back pain recommend exercise but note that there is no evidence that one form of exercise is superior to another. The European guideline advises against exercise that requires expensive training and machines. The one area of therapy that is contentious is the use of spinal manipulation. Some guidelines do not recommend the treatment (e.g. Spanish, Australian), some advise that it is optional (e.g. Austrian, Italian) and some suggest a short course for those who do not respond to the first line of treatment (e.g. US, the Netherlands). For some it is optional only in the first weeks of an episode in acute low back pain (e.g. Canada, Finland, Norway, Germany, New Zealand). The French guideline advises that there is no evidence to recommend one form of manual therapy over another.
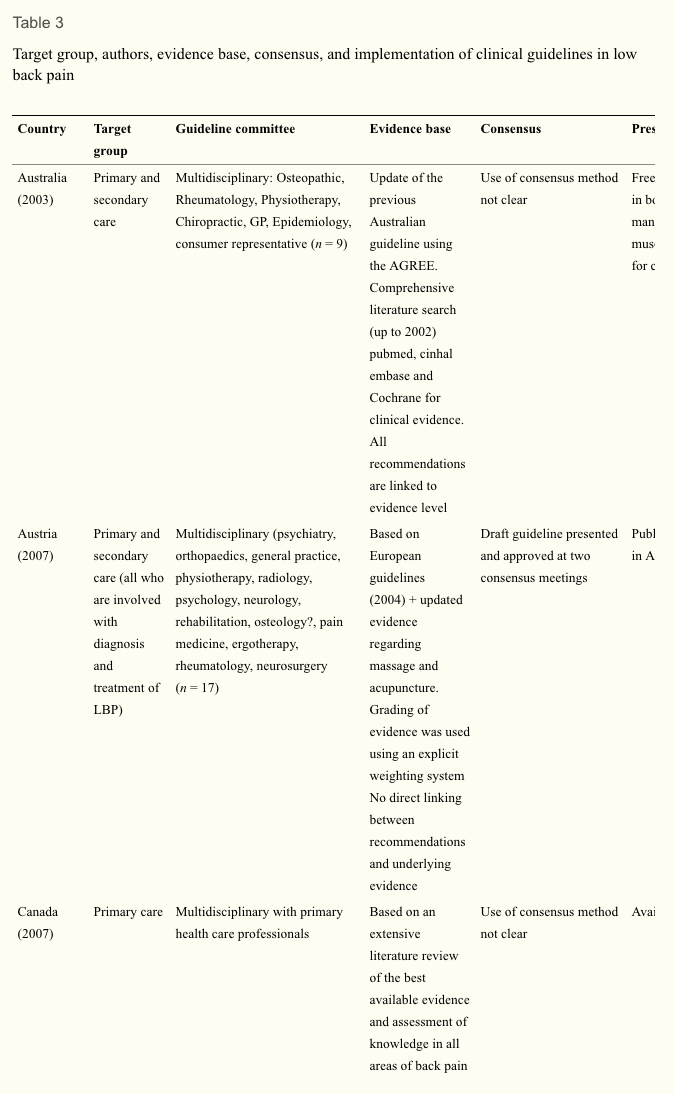
Setting. Table 3 shows some background variables related to the development of the guidelines in the various countries. Most of the guidelines focus on primary care though some also include secondary care. The Spanish guideline is written for health professions that treat low back pain.
Guideline committee. The various committees responsible for the development and publication of guidelines appear to be different in size and in the professional disciplines involved. Most committees are characterised by their multidisciplinary membership. These usually included primary care physicians, physical and manual therapists, orthopaedic surgeons, rheumatologists, radiologists, occupational and rehabilitation physicians. The number of members varied from 7 to 31. Only three committees included consumer representation (Australia, New Zealand, the Netherlands).
Evidence-based review. All guidelines are more or less based on a comprehensive literature search, including Cochrane Library, Medline, Embase. Some committees (Austria, Germany, Spain) based their recommendations, entirely or in part, on the European guidelines. Most guidelines use an explicit weighting of the strength of the evidence.
The Dutch, UK, European, Finnish, German, Norwegian and Australian guidelines give direct links between the actual recommendations and the evidence (via specific references) on which the recommendations are based. Other guidelines do not present a direct link but state that for recommendation there is at least moderate or fair evidence (New Zealand, US). Most committees use consensus methods, mostly by group discussions when the evidence was not convincing or not available.
Presentation and implementation. The activities related to the publication and dissemination of the various guidelines show some differences and some similarities. In most cases, the guidelines are accompanied by easily accessible summaries for practitioners and booklets for patients. Systematic implementation activities are rare. In most cases, the printed versions of the guidelines are published in national journals and/or disseminated through professional organisations to the target practitioners. Most guidelines are available on the websites of participating organisation. In many countries, regular updates of the guidelines are planned with time horizons of 3�5 years.
Discussion
In the past decade many countries have issued (updated) clinical guidelines for the management of low back pain. In general these guidelines provide similar advice on the management of low back pain. Common recommendations are the diagnostic triage of patients with low back pain, restricted use of radiographs, advice on early and progressive activation of patients, and the related discouragement of bed rest. The recognition of psychosocial factors as a risk factor for chronicity is also consistent across all guidelines, though with varying emphasis and detail. There are also differences in the recommendations provided by the guidelines, but these are few and probably less than could expected for different health care systems and cultures. One of the reasons for the similarity of the guidelines might be that guideline committees are usually aware of the content of other guidelines and are motivated to produce similar recommendations that are deemed sensible and relevant. In some instances the guidelines are a national adaptation (e.g. in Spain) of the European guidelines.
We do not present an exhaustive overview of all clinical guidelines available, but focused on national multidisciplinary guidelines. This enables a reasonable comparison of recommended approaches across countries. A limitation is thus that not all available guidelines, including mono-disciplinary guidelines, are included.
Use of Available Evidence
Most reviews are based on extensive literature reviews. Cochrane reviews are frequently used, comprehensive searches in databases such as Medline, Embase and PEDro. Increasingly the literature reviews of other and previous guidelines are used as starting point for the (additional) searches. Most committees also use some kind of weighting system and rating of the evidence. There is some variation in the way the recommendations are presented. In some guidelines all the recommendations are directly linked with references to the supporting evidence, and in others a general remark is made that for all recommendations that there is at least moderate evidence available.
Differences in Recommendations
Recommendations about the prescription of analgesic medication remain fairly consistent. Most guidelines recommend paracetamol as the first option and nonsteroidal anti-inflammatory preparations as the second option. Further recommendations about other drugs like opioids, muscle relaxants and benzodiazepines and antidepressants vary quite considerably. Part of these variations might reflect the setting and custom in different countries. Since all the guidelines were issued within a relative short time frame, the availability of underlying evidence did not vary much.
The recommendations regarding spinal manipulation continue to show some variation. In some guidelines manipulation is recommended, or presented as a therapeutic option, usually for short-term benefit, but others do not recommend it. This holds true for acute as well as chronic low back pain. The reasons for these differences remain speculative. Probably the underlying evidence is not strong enough to result in similar recommendations regarding manipulation across all guidelines, leaving the committees some more room for interpretation, but also local or political reasons may be involved.
There is now relatively large consensus across the various guidelines that specific back exercises (as opposed to the advice to stay active, including for example walking, cycling) are not recommended for patients with acute low back pain. At the same time back exercises are recommended in chronic low back pain. Most guidelines do not recommend a particular type of exercises for chronic low back pain, but some state that they should be intense.
Recommendations in guidelines are based not only on scientific evidence but also on consensus and discussion in the guideline committees. Usually it is stated that consensus was based on group discussion, but the details of these discussions are seldom reported. It is also generally unclear which recommendations are based mainly on scientific evidence and which are based on (mainly) consensus.
There is little information on whether cost-effectiveness played an important role as a basis for the recommendation in a guideline. Of course, there are not yet many cost-effectiveness studies available [23], but it is not fully clear to what extent the published studies were used.
Most guidelines state that the prognosis of an episode of low back pain is good. This holds especially true for patients with acute episodes of low back pain. For patients presenting with a longer duration with low back pain or with recurrent low back pain the prognosis may be less favourable. More individualised and precise estimates of the prognosis of an episode of low back pain may be desirable in the future.
Few Changes in Management Recommendations Over Time
This update showed that overall the recommendations in the current guidelines regarding diagnosis and treatment of low back pain did not change substantially compared to the guidelines issued about a decade ago. This may well illustrate the lack of new evidence showing better results with new diagnostic and therapeutic approaches and/or new evidence showing the inefficacy of existing interventions. A less nihilistic view could be that already a decade ago the most valid recommendations for the management of low back pain were identified. Some may argue that this is indeed the case, and that much more effort should now be given to implementation of guidelines (see below).
Some recommendations did change over time. We now see diagnostic recommendations appearing concerning the value of MRI and CT scans (i.e. in relation to exclusion and further diagnosis of red flags and serious spinal disorders). However, these recommendations are not yet strong, possibly because there are not many diagnostic studies available evaluating the value of MRI in patients with low back pain. Also, the recommendations regarding the assessment of psychosocial risk factors for chronicity are more firm in the current guidelines than that a decade ago. This reflects the insight of the importance of these risk factors for the development of chronicity and future disability. At the same time we must conclude that we are not yet very successful in effective screening of the patients at risk and subsequent therapeutic management of them [24].
Most apparent changes regarding therapeutic interventions include the advice to continue work (despite having low back pain) and or return to work as soon as possible. There are now more recommendations of second line medications such as antidepressants, opioids, benzodiazepines and compound medications. But these recommendations are not consistent across countries, potentially because of weak underlying evidence. There are now also more firm recommendations in favour of exercise therapy in patients with subacute and chronic low back pain. The latter is partly due to the fact that currently more guidelines include recommendation for the management of chronic low back pain as compared to a decade ago. Finally, the reasons and options for referral within primary care and secondary care are now more explicitly presented. It appears that the global approach regarding the management of low back pain remained largely unchanged in the past decade, although some refinements have been suggested.
Implementation
The extent to which currently available guidelines are used and followed in the various countries remains largely unknown. A few studies evaluating various implementation strategies for low back pain guidelines show that changing clinical practice is not an easy task [25, 26]. The publication and dissemination of guidelines alone is usually not enough to change the behaviour of health care providers [27]. The development of effective implementation strategies in this area remains a challenge.
Future Developments in Research and Guideline Development
The present study was primary aimed at presenting an update of the current clinical guidelines for the management of low back pain in primary care. Clinical guidelines focused at secondary care settings, occupational care settings, or specific subgroups of patients with lumbosacral radicular syndrome were not considered. Separate studies need to be undertaken to present an overview for these settings.
We assessed various aspects of the guideline development in Table 3. A formal assessment of the quality, e.g. with the AGREE instrument was not included. This was the topic of a separate paper which concluded that the quality of the guidelines indeed has improved over time [7].
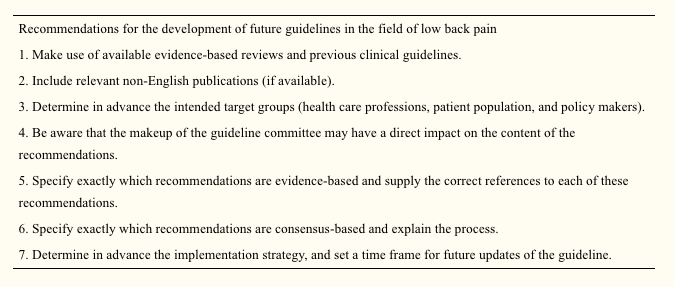
The development of future guidelines in this field may benefit from previous experiences, evidence-based reviews, and various (inter) national guidelines as presented in this overview. The previous review of clinical guidelines listed the following recommendations (slightly modified) for the development of future guidelines in this field. Similar to a recent review on the quality of guidelines [7], this review shows that the quality of guidelines has improved over time and some of the recommendations have been followed. This includes recommendations 1, 3, and 4 (see below). For others, there still is room for improvement Recommendation 2 is not consistently applied. Recommendations 5 and 6 have improved over time, but not all recommendations in the guidelines are directly linked to the underlying evidence, and the process of the consensus methods used is not well described. Finally, the implementation strategies and the time frame of future updates are not well presented.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
Based upon search of PEDro database April 29, 2009.
In conclusion,�low back pain is a prevalent medical complaint which affects million of people in the United States alone. Although it may seem difficult to diagnose low back pain because of its many possible causes, a chiropractor, or doctor of chiropractic, can properly diagnose the source of a patient’s low back pain to treat as well as prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care utilizes spinal adjustments and manual manipulations, among other treatment methods, to carefully restore the original alignment of the spine, allowing the human body to naturally heal itself. The purpose of the article above is to present updated treatment guidelines fot the management of low back pain in a primary care setting.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Koes BW, Tulder MW, Thomas S. Diagnosis and treatment of low back pain.�BMJ.�2006;332(7555):1430�1434. doi: 10.1136/bmj.332.7555.1430.�[PMC free article]�[PubMed]�[Cross Ref]
2.�Pengel L, Herbert R, Maher CG, Refshauge K. Acute low back pain: systematic review of its prognosis.�BMJ.�2003;327:323�327. doi: 10.1136/bmj.327.7410.323.�[PMC free article]�[PubMed]�[Cross Ref]
3.�Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, York J, Das A, McAuley JH. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study.�BMJ.�2008;337:171. doi: 10.1136/bmj.a171.�[PMC free article]�[PubMed]�[Cross Ref]
4.�Australian Institute of Health and Welfare (2004) Australia�s Health 2004. AIHW, Canberra
5.�Spitzer W. Scientific approach to the assessment and management of activity-related spinal disorders.�Spine.�1987;12:1�58. doi: 10.1097/00007632-198701000-00001.�[PubMed]�[Cross Ref]
6.�Koes BW, Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine.�2001;26:2504�2513. doi: 10.1097/00007632-200111150-00022.�[PubMed]�[Cross Ref]
7.�Bouwmeester W, Enst A, Tulder MW. Quality of low back pain guidelines improved.�Spine.�2009;34:2562�2567. doi: 10.1097/BRS.0b013e3181b4d50d.�[PubMed]�[Cross Ref]
8.�Evidence-based management of acute musculoskeletal pain.�Bowen Hills: Australian Academic Press; 2003.
9.�Friedrich M, Likar R. Evidenz- und konsensusbasierte �sterreichische Leitlinien f�r das Management akuter und chronischer unspezifischer Kreuzschmerzen.�Wien Klin Wochenschr.�2007;119(5�6):189�197. doi: 10.1007/s00508-006-0754-3.�[PubMed]�[Cross Ref]
11.�Tulder MW, Becker A, Bekkering T, et al. European guidelines for the management of acute low back pain in primary care.�Eur Spine J.�2006;15(Suppl 2):S169�S191. doi: 10.1007/s00586-006-1071-2.[PMC free article]�[PubMed]�[Cross Ref]
12.�Airaksinen O, Brox JI, Cedraschi C, et al. European guidelines for the management of chronic non-specific low back pain.�Eur Spine J.�2006;15(2):S192�S300. doi: 10.1007/s00586-006-1072-1.[PMC free article]�[PubMed]�[Cross Ref]
13.�Malmivaara A, Erkintalo M, Jousimaa J, Kumpulainen T, Kuukkanen T, Pohjolainen T, Seitsalo S, �sterman H (2008) Aikuisten alaselk�sairaudet. (Low back pain among adults. An update within the Finnish Current Care guidelines). Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis, Fenniae. Duodecim 124:2237�2239
14.�Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) Guidelines department, diagnosis and management of acute low back pain (<3�months) with or without sciatica & diagnosis, management and follow-up of patients with chronic low back pain, Paris.�www.anaes.fr�or�www.sante.fr
15.�Drug Committee of the German Medical Society (2007) Recommendations for treatment of low back pain [in German]. K�ln, Germany
16.�Negrini S, Giovannoni S, Minozzi S, et al. Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guidelines.�Euro Medicophys.�2006;42(2):151�170.�[PubMed]
17.�National Health Committee (2004) National Advisory Committee on Health and Disability, Accident Rehabilitation and Compensation Insurance Corporation. New Zealand Acute Low back pain Guide. Wellington, New Zealand
18.�Laerum E, Storheim K, Brox JI. New clinical guidelines for low back pain.�Tidsskr Nor Laegeforen.�2007;127(20):2706.�[PubMed]
19.�Spain, the Spanish Back Pain Research Network (2005) Guia de practica clinica. Lumbalgia Inespecifica. Version espnola de la Guia de Practica Clinica del Programa Europeo COST B13
20.�The Dutch Institute for Healthcare Improvement (CBO) (2003) Clinical guideline for non-specific low back pain [in Dutch]
22.�Chou R, Qaseem A, Snow V, et al. Clinical Efficacy Assessment Subcommittee of the American College of Physicians American College of Physicians American Pain Society Low back pain Guidelines Panel Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society.�Ann Intern Med.�2007;147(7):478�491.�[PubMed]
23.�Roer N, Goossens ME, Evers SM, Tulder MW. What is the most cost-effective treatment for patients with low back pain? A systematic review.�Best Pract Res Clin Rheumatol.�2005;19(4):671�684. doi: 10.1016/j.berh.2005.03.007.�[PubMed]�[Cross Ref]
24.�Jellema P, Windt DA, Horst HE, Blankenstein AH, Bouter LM, Stalman WA. Why is a treatment aimed at psychosocial factors not effective in patients with (sub)acute low back pain?�Pain.�2005;118(3):350�359. doi: 10.1016/j.pain.2005.09.002.�[PubMed]�[Cross Ref]
25.�Bekkering GE, Tulder MW, Hendriks EJM, Koopmanschap MA, Knol DL, Bouter LM, Oostendorp RAB. Implementation of clinical guidelines on physical therapy for patients with low back pain: randomized trial comparing patient outcomes after a standard and active implementation strategy.�Phys Ther.�2005;85(6):544�555.�[PubMed]
26.�Engers AJ, Wensing M, Tulder MW, Timmermans A, Oostendorp RA, Koes BW, Grol R. Implementation of the Dutch low back pain guideline for general practitioners: a cluster randomized controlled trial.�Spine.�2005;30(6):595�600. doi: 10.1097/01.brs.0000155406.79479.3a.�[PubMed][Cross Ref]
27.�Becker A, Leonhardt C, Kochen MM, Keller S, Wegscheider K, Baum E, Donner-Banzhoff N, Pfingsten M, Hildebrandt J, Basler HD, Chenot JF. Effects of two guideline implementation strategies on patient outcomes in primary care: a cluster randomized controlled trial.�Spine.�2008;33(5):473�480. doi: 10.1097/BRS.0b013e3181657e0d.�[PubMed]�[Cross Ref]
Chiropractic care is a well-known alternative treatment option commonly utilized to treat symptoms of sciatica. Sciatica is characterized as radiating pain that originates in the lower back which then travels down the buttocks and hips into the leg and foot as a result of the compression of the sciatic nerve. Symptoms generally develop on a single side of the body, however, sciatica may occur on both sides of the human body. Sciatic nerve pain can vary in frequency and intensity from person to person and it’s commonly described as a dull, sharp, pins and needles sensation similar to electric shocks.
Other symptoms include, burning, numbness and tingling sensations. Common disorders known to cause sciatic nerve pain include, piriformis syndrome or compression caused by the inflammation of the piriformis muscle, subluxations or misalignments of the lumbar spine, bulging or herniated discs, pregnancy, tumors and non-spinal disorders like diabetes and constipation. Because many disorders can cause sciatica, the proper diagnosis of the source of the symptoms of each individual is essential towards every patient’s treatment requirements. Diagnostic testing for sciatic nerve pain includes x-ray, MRI, CT scan and/or electrodiagnostic tests. These examinations can help determine possible contraindications to chiropractic care.
Chiropractic care focuses on the diagnosis, treatment and prevention of a variety of injuries and/or conditions affecting the musculoskeletal and nervous system by carefully restoring the original alignment of the spine through the use of spinal adjustments and manual manipulations, among other types of treatment methods. The purpose of chiropractic care is to naturally increase the human body’s ability to heal itself without the need for drugs/medication and/or surgery. A chiropractor can provide a variety of treatment methods depending on the source of a patient’s sciatic nerve pain. A common treatment plan for sciatic nerve pain performed by a chiropractor may include spinal adjustments and manual manipulations, ice/cold therapies to reduce inflammation, ultrasound for increasing circulation, TENS or transcutaneous electrical nerve stimulation and lifestyle modifications, such as nutritional advice, fitness recommendations and sleep scheduling. Other treatment methods commonly utilized by a chiropractor to treat sciatica include, flexion-distraction therapy, spinal decompression therapy and the McKenzie therapy.
Flexion-distraction therapy is a gentle procedure utilized for neck and back pain that increases the intervertebral disc height, allowing each disc to assume its central position in order to decrease tension, relieve irritation of the spinal nerve and improve circulation. Flexion-distraction therapy can restore body functions as well as relieve pain. Spinal decompression therapy involves intermittent stretching of the spine in a controlled manner utilizing a traction table or similar motorized device to create a negative intradiscal pressure in order to relieve back pain and/or radiating pain by promoting the passage of healing nutrients into the disc and providing a better healing environment for bulging or herniated discs. And finally, the McKenzie therapy is a standardized approach to both the assessment and treatment of sciatica. The treatment method requires a patient to participate in a series of physical activities in order to evaluate the patient’s pain response and determine the health issue. The McKenzie therapy then utilizes that information to develop a fitness routine with a focus on alleviating painful symptoms.
Although chiropractic care is a safe and effective alternative treatment option commonly utilized to treat symptoms of sciatica, sciatica can be caused by disorders beyond the limit of chiropractic care. If a doctor of chiropractic, or chiropractor, determines that a patient’s disorder requires treatment from another type of specialist, they may refer the individual to another healthcare professional for further treatment. In several cases, the referring chiropractor may continue chiropractic care while co-managing the patient’s treatment with the other specialist. Furthermore, the purpose of the following article is to demonstrate a variety of treatment guidelines on the diagnosis and treatment of sciatica. However, because the information regarding the prevalence of the source of sciatica and its response to specific treatment methods is lacking, further research studies are still required to determine the efficiency of the treatment guidelines mentioned below.
Diagnosis and Treatment of Sciatica
Sciatica affects many people. The most important symptoms are radiating leg pain and related disabilities. Patients are commonly treated in primary care but a small proportion is referred to secondary care and may eventually have surgery. Many synonyms for sciatica appear in the literature, such as lumbosacral radicular syndrome, ischias, nerve root pain, and nerve root entrapment.
Summary Points
Most patients with acute sciatica have a favourable prognosis but about 20%-30% have persisting problems after one or two years
The diagnosis is based on history taking and physical examination
Imaging is indicated only in patients with �red flag� conditions or in whom disc surgery is considered
Passive (bed rest) treatments have been replaced with more active treatments
Consensus is that initial treatment is conservative for about 6-8 weeks
Disc surgery may provide quicker relief of leg pain than conservative care but no clear differences have been found after one or two years
In about 90% of cases sciatica is caused by a herniated disc with nerve root compression, but lumbar stenoses and (less often) tumours are possible causes. The diagnosis of sciatica and its management varies considerably within and between countries�for example, the surgery rates for lumbar discectomy vary widely between countries.[w1] A recent publication confirmed this large variation in disc surgery, even within countries.[1] This may in part be caused by a paucity of evidence on the value of diagnostic and therapeutic interventions and a lack of clear clinical guidelines or reflect differences in healthcare and insurance systems. This review presents the current state of science for the diagnosis and treatment of sciatica.
Sources and Selection Criteria
We identified systematic reviews in the Cochrane Library evaluating the effectiveness of conservative and surgical interventions for sciatica. Medline searches up to December 2006 were carried out to find other relevant systematic reviews on the diagnosis and treatment of low back pain. Keywords were sciatica, hernia nuclei pulposi, ischias, nerve root entrapment, systematic review, meta-analysis, diagnosis, and treatment. In addition we used our personal files for other references, including publications of recent randomised clinical trials. Finally we checked the availability of clinical guidelines.
Dr. Alex Jimenez’s Insight
Sciatica is medically defined as a collective group of symptoms, rather than a single injury and/or condition, commonly characterized by radiating pain along the sciatic nerve in the lower back, which runs down the buttocks and into both legs and feet. Sciatica generally occurs along a single side of the body although it can rarely affect both sides of the human body. Sciatic nerve pain can manifest as a result of a variety of injuries and/or conditions, such as a bulging or herniated disc, which can often make it difficult for healthcare professionals to properly treat it. The role of a chiropractor is to determine the source of a patient’s sciatica in order to utilize the best treatment method for their specific health issue. A chiropractor, or doctor of chiropractic, will commonly use spinal adjustments and manual manipulations, among other treatment methods, to carefully restore the original integrity of the spine and improve symptoms of sciatica. Chiropractic care can increase the human body’s potential to naturally heal itself.
Who Gets Sciatica?
Exact data on the incidence and prevalence of sciatica are lacking. In general an estimated 5%-10% of patients with low back pain have sciatica, whereas the reported lifetime prevalence of low back pain ranges from 49% to 70%.[w2] The annual prevalence of disc related sciatica in the general population is estimated at 2.2%.[2] A few personal and occupational risk factors for sciatica have been reported, including age, height, mental stress, cigarette smoking, and exposure to vibration from vehicles.[2, 3, w2] Evidence for an association between sciatica and sex or physical fitness is conflicting.[2, 3, w2]
Risk Factors for Acute Sciatica[3, w2]
Personal Factors
Age (peak 45-64 years)
Increasing risk with height
Smoking
Mental stress
Occupational Factors
Strenuous physical activity�for example, frequent lifting, especially while bending and twisting
Driving, including vibration of whole body
How is Sciatica Diagnosed?
Sciatica is mainly diagnosed by history taking and physical examination. By definition patients mention radiating pain in the leg. They may be asked to report the distribution of the pain and whether it radiates below the knee and drawings may be used to evaluate the distribution. Sciatica is characterised by radiating pain that follows a dermatomal pattern. Patients may also report sensory symptoms.
Physical examination largely depends on neurological testing. The most applied investigation is the straight leg raising test or Las�gue’s sign. Patients with sciatica may also have low back pain but this is usually less severe than the leg pain. The diagnostic value of history and physical examination has not been well studied.[4] No history items or physical examination tests have both high sensitivity and high specificity. The pooled sensitivity of the straight leg raising test is estimated to be 91%, with a corresponding pooled specificity of 26%.[5] The only test with a high specificity is the crossed straight leg raising test, with a pooled specificity of 88% but sensitivity of only 29%.[5] Overall, if a patient reports the typical radiating pain in one leg combined with a positive result on one or more neurological tests indicating nerve root tension or neurological deficit the diagnosis of sciatica seems justified. Below shows the signs and symptoms that help to distinguish between sciatica and non-specific low back pain.
Indicators for Sciatica[w5]
Unilateral leg pain greater than low back pain
Pain radiating to foot or toes
Numbness and paraesthesia in the same distribution
Straight leg raising test induces more leg pain
Localised neurology�that is, limited to one nerve root
What is the Value of Imaging?
Diagnostic imaging is only useful if the results influence further management. In acute sciatica the diagnosis is based on history taking and physical examination and treatment is conservative (non-surgical). Imaging may be indicated at this stage only if there are indications or �red flags� that the sciatica may be caused by underlying disease (infections, malignancies) rather than disc herniation.
Diagnostic imaging may also be indicated in patients with severe symptoms who fail to respond to conservative care for 6-8 weeks. In these cases surgery might be considered and imaging used to identify if a herniated disc with nerve root compression is present and its location and extent. It is important as part of the decision to operate that the clinical findings and symptoms correspond well with the scan findings. This is especially relevant because disc herniations identified by computed tomography or magnetic resonance imaging are highly prevalent (20%-36%) in people without symptoms who do not have sciatica.[6, w3] In many people with clinical symptoms of sciatica no lumbar disc herniations are present on scans.[7, 8] At present no one type of imaging method shows a clear advantage over others. Although some authors favour magnetic resonance imaging above other imaging techniques because computed tomography has a higher radiation dose or because soft tissues are better visualised,[9, 10] evidence shows that both are equally accurate at diagnosing lumbar disc herniation.[11] Radiography for the diagnosis of lumbar disc herniation is not recommended because discs cannot be visualised by x rays.[11]
What is the Prognosis?
In general the clinical course of acute sciatica is favourable and most pain and related disability resolves within two weeks. For example, in a randomised trial that compared non-steroidal anti-inflammatory drugs with placebo for acute sciatica in primary care 60% of the patients recovered within three months and 70% within 12 months.[12] About 50% of patients with acute sciatica included in placebo groups in randomised trials of non-surgical interventions reported improvement within 10 days and about 75% reported improvement after four weeks.[13] In most patients therefore the prognosis is good, but at the same time a substantial proportion (up to 30%) continues to have pain for one year or longer.[12, 13]
What is the Efficacy of Conservative Treatments for Sciatica?
Conservative treatment for sciatica is primarily aimed at pain reduction, either by analgesics or by reducing pressure on the nerve root. A recent systematic review found that conservative treatments do not clearly improve the natural course of sciatica in most patients or reduce symptoms.[14] Adequately informing patients about the causes and expected prognosis may be an important part of the management strategy. However, educating patients about sciatica has not been specifically investigated in randomised controlled trials.
The information below summarises the evidence of effectiveness for commonly available conservative treatments for sciatica, including injection therapy. Strong evidence of effectiveness is lacking for most of the available interventions. Little difference in effect on pain and functional status has been shown between bed rest and advice on staying active.[15] As a result of this finding, bed rest�for a long time the mainstay of treatment for sciatica�is no longer widely recommended.[w2, w4] Analgesics, non-steroidal anti-inflammatory drugs, and muscle relaxants do not seem to be more effective than placebo in reducing symptoms. Evidence for opioids and various compound drugs is lacking. A systematic review reported that no evidence exists for traction, non-steroidal anti-inflammatory drugs, intramuscular steroids, or tizanidine being superior to placebo.[13] This review suggested that epidural injections of steroid might be effective in patients with acute sciatica.[13] However a more recent systematic review of a larger number of randomised trials reported that there was no evidence of positive short term effects of corticosteroid injections and that the long term effects were unknown.[14] The same systematic review reported that active physical therapy (exercises) seemed not to be better than inactive (bed rest) treatment and other conservative treatments, such as traction, manipulation, hot packs, or corsets).[14]
Levels of Evidence for Conservative Treatments for Sciatica
Bed rest (trade-off)
Staying active, in contrast to bed rest (likely to be beneficial)
Surgical intervention for sciatica focuses on removal of disc herniation and eventually part of the disc or on foraminal stenosis, with the purpose of eliminating the suspected cause of the sciatica. Treatment is aimed at easing the leg pain and corresponding symptoms and not at reducing the back pain. Consensus is that a cauda equina syndrome is an absolute indication for immediate surgery. Elective surgery is the choice for unilateral sciatica. Until recently only one relatively old randomised trial was available that compared surgical intervention with conservative treatment for patients with sciatica.[16] This study showed that surgical intervention had better results after one year, whereas after four and 10 years of follow-up no significant differences were found.[16]
A Cochrane review summarised the available randomised clinical trials evaluating disc surgery and chemonucleolysis.[17] In chemonucleolysis the enzyme chymopapain is injected in the discus with the purpose of shrinking the nucleus pulposus. The review reported better results with disc surgery than with chemonucleolysis in patients with severe sciatica of relatively long duration varying from more than four weeks to more than four months. Chemonucleolysis was more effective than placebo. Indirectly therefore the review suggested that disc surgery is more effective than placebo. On the basis of data from three trials the authors concluded that evidence is considerable that surgical discectomy provides effective clinical relief for carefully selected patients with sciatica as a result of lumbar disc prolapse that fails to resolve with conservative care. A recent review came to the same conclusion.[18] The Cochrane review further concluded that the long term effects of surgical intervention are unclear and that evidence on the optimal timing of surgery is also lacking.[17]
Randomised Controlled Trials not yet Included in Systematic Reviews
Two additional randomised controlled trials have been published comparing disc surgery with conservative treatment. One trial (n=56) compared microdiscectomy with conservative treatment in patients who had had sciatica for six to 12 weeks.[19] Overall, no significant differences were found for leg pain, back pain, and subjective disability over two years of follow-up. Leg pain, however, seemed to initially improve more rapidly in patients in the discectomy group. The large spine patient outcomes research trial (a randomised trial) and related observational cohort study was carried out in the United States.[20, 21] Patients with sciatica for at least six weeks and confirmed disc herniation were invited to participate in either a randomised trial or an observational cohort study. Patients in the trial were randomised to disc surgery or to conservative care. Patients in the cohort study received disc surgery or conservative care based on their preference. In the randomised trial (n=501) both treatment groups improved substantially over two years for all primary and secondary outcome measures. Small differences were found in favour of the surgery group, but these were not statistically significant for the primary outcome measures. Only 50% of the patients randomised to surgery received surgery within three months of inclusion compared with 30% randomised to conservative care. After two years of follow-up 45% of patients in the conservative care group underwent surgery compared with 60% in the surgery group.[20]
The observational cohort included 743 patients. Both groups improved substantially over time, but the surgery group showed significantly better results for pain and function compared with the conservative group. The authors did mention caution in interpreting the findings because of potential confounding by indication and because outcome measures were self reported.[21]
The results indicate that both conservative care and disc surgery are relevant treatment options for patients with sciatica of at least six weeks’ duration. Surgical intervention may provide quicker relief of symptoms compared with conservative care, but no large differences have been found in success rate after one or two years of follow-up. Patients and doctors may thus weigh the benefits and harms of both options to make individual choices. This is especially relevant because patients’ preference for treatment may have a direct positive influence on the magnitude of the treatment effect.
What are the Recommendations in Clinical Guidelines?
Although in many countries clinical guidelines are available for the management of non-specific low back pain this is not the case for sciatica.[22] Below shows the recommendations for sciatica (lumbosacral radicular syndrome) in clinical guidelines recently issued by the Dutch College of General Practice.[w4] After excluding specific diseases on the basis of red flags, sciatica is diagnosed on the basis of history taking and physical examination. Initial treatment is conservative, with a strong focus on patient education, advice to stay active, continuing daily activities, and adequate treatment for pain. In this phase imaging has no role. Referral to a medical specialist�for example, neurologist, rheumatologist, spine surgeon�is indicated in patients whose symptoms do not improve after conservative treatment for at least 6-8 weeks. In these referred cases surgery may be considered. Immediate referral is indicated in cases with a cauda equina syndrome. Acute severe paresis or progressive paresis are also reasons for referral (within a few days).
Clinical Guideline for Diagnosis and Treatment of Sciatica from Dutch College of General Practice[w4]
Diagnosis
Check for red flag conditions, such as malignancies, osteoporotic fractures, radiculitis, and cauda equina syndrome
Take a history to determine localisation; severity; loss of strength; sensibility disorders; duration; course; influence of coughing, rest, or movement; and consequences for daily activities
Carry out a physical examination, including neurological testing�for example, straight leg raising test (Las�gue’s sign)
Carry out the following tests in cases with a dermatomal pattern, or positive result on straight leg raising test, or loss of strength or sensibility disorders: reflexes (Achilles or knee tendon), sensibility of lateral and medial sides of feet and toes, strength of big toe during extension, walking on toes and heel (left-right differences), crossed Las�gue’s sign
Imaging or laboratory diagnostic tests are only indicated in red flag conditions but are not useful in cases of suspected disc herniation
Treatment
Explain cause of the symptoms and reassure patients that symptoms usually diminish over time without specific measures
Advise to stay active and continue daily activities; a few hours of bed rest may provide some symptomatic relief but does not result in faster recovery
Prescribe drugs, if necessary, according to four steps: (1) paracetamol; (2) non-steroidal anti-inflammatory drugs; (3) tramadol, paracetamol, or non-steroidal anti-inflammatory drug in combination with codeine; and (4) morphine
Refer to neurosurgeon immediately in cases of cauda equina syndrome or acute severe paresis or progressive paresis (within a few days)
Refer to neurologist, neurosurgeon, or orthopaedic surgeon for consideration of surgery in cases of intractable radicular pain (not responding to morphine) or if pain does not diminish after 6-8 weeks of conservative care
Promising Developments
More evidence based information has become available on the efficacy of surgical care compared with conservative care for patients with sciatica. Although evidence is limited, initial findings suggest no important differences in long term (one or two years) effect between these two approaches. This finding may be partly explained by patients who initially received conservative care later undergoing disc surgery. In all available studies it seems that a substantial proportion of patients improve over time. This holds true for patients undergoing surgery or receiving conservative care. Patients undergoing disc surgery are more likely to get quicker relief of leg symptoms than patients receiving conservative care. If symptoms do not improve after 6-8 weeks patients may opt for disc surgery. Those who are hesitant about surgery and can cope with their symptoms may opt for continued conservative care. Patient preference is therefore an important feature in the decision process.
Since the mid-1990s a switch has occurred in the management of sciatica from passive treatments, such as bed rest, to a more active approach, with patients being advised to continue their daily activities as much as possible.
Future Research
More information is needed on the importance of clinical signs and symptoms for the prognosis of sciatica and the response to treatment. This includes the value of size and location of the disc herniation, visible nerve root compression, sequestration, and the results of history taking and physical and neurological examinations. Subgroup analysis in a Finnish trial showed that discectomy was superior to conservative treatment in patients with disc herniation at L4-5.[23] No strong evidence exists for or against the efficacy of many of the available conservative treatments. Much progress can be achieved here. Questions remain about the efficacy of analgesics for sciatica and the value of physical therapy and of patient education and counselling. No trial has yet evaluated the effectiveness of behavioural treatment and multidisciplinary treatment programmes.
Tumour necrosis factor ? has been identified in animal and human studies as one factor in the development of sciatica.[23, 24] The first randomised trial evaluating a tumour necrosis factor ? antagonist in patients with sciatica did not find a positive result.[25]
Additional Educational Resources
BMJ Clinical Evidence (www.clinicalevidence.org)�Up to date evidence for clinicians on the benefits and harms of treatments for a variety of disorders
Cochrane Back Review Group (www.cochrane.iwh.on.ca)�Activities of review group responsible for writing systematic Cochrane reviews on the efficacy of treatments for low back pain and sciatica
Low back pain: guidelines for its management (www.backpaineurope.org)�Recently issued guidelines for the management of low back pain and sciatica from the European Commission Research Directorate General
A Patient’s Perspective (A)
After an episode of lumbago during a vacation I continuously had low back pain and tingling feet for about nine months. Then suddenly my right foot started to hurt badly and after a while the pain became so severe that I was unable to leave my house. The specialist ordered an MRI (magnetic resonance imaging) scan and it revealed a large lumbar disc herniation. Since it only got worse after that I decided to have surgery.
After the operation I recovered quickly and the back pain and leg pain were completely gone. I soon was able to go back to work and rebuild my social life. Unfortunately after a couple of months the low back pain and the other symptoms returned, although not as severe as before surgery. A new MRI scan now revealed two small disc herniations and two bad intervertebral discs. The specialist told me that it was too early for a second operation.
Now it is unclear to me what the doctor can do about it and I don’t even know which measures I can take myself. The constant back and leg pain are greatly interfering with my work and my social life. I sometimes feel like an elderly person because of my physical limitations. I try to stay positive, but it is hard to cope with the uncertainty.
C Penning, aged 32, Rotterdam
A Patient’s Perspective (B)
My complaints started about four months ago with pain in the lower back. Soon after the pain radiated into my legs, for which I went to my general practitioner. His analysis was no herniated disc. A muscle relaxant in combination with referral to a physiotherapist would reduce the symptoms. Three weeks of physiotherapy followed by several treatments by a chiropractor did not provide any symptom relief. In fact the symptoms became worse�especially during walking and standing. Lying down and cycling were much better tolerated. Additional complaints were reduced strength in the left leg, not being able to stand on the heel or toes, a cold feeling in the lower leg at the end of the day, while in the morning it felt like standing in a bunch of needles.
About one month ago a neurologist diagnosed a herniated disc on the right side based on an MRI scan that was taken. However, this could not explain the symptoms in the left leg. The symptoms in the left leg could be due to spinal stenosis. The complaints were not severe enough to recommend surgery and the neurologist told me that a substantial improvement was to be expected within a period of 3-4 months. His advice was to continue normal daily activities as much as possible. At present (one month later) I feel some improvement of my symptoms.
Contributors: BWK wrote the first draft. MWvT and WCP critically appraised and improved the manuscript. BWK is guarantor.
Competing interests: None declared.
Provenance and peer review: Commissioned; peer reviewed.
In conclusion,�chiropractic care is a popular alternative treatment option commonly utilized to treat sciatica symptoms. While sciatic nerve pain can occur due to a variety of injuries and/or conditions, the purpose of chiropractic care is to determine the source of a patient’s sciatica in order to properly treat their symptoms using a variety of treatment methods. The article above demonstrates several treatment guidelines for sciatica, however, further research studies are required. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES. United States’ trends and regional variations in lumbar spine surgery: 1992-2003.�Spine�2006;31:2707-14.�[PMC free article]�[PubMed]
2.�Younes M, Bejia I, Aguir Z, Letaief M, Hassen-Zroer S, Touzi M, et al. Prevalence and risk factors of disc-related sciatica in an urban population in Tunisia.�Joint Bone Spine�2006;73:538-42.�[PubMed]
3.�Miranda H, Viikari-Juntera E, Martikainen R, Takala E, Riihimaki H. Individual factors, occupational loading, and physical exercise as predictors of sciatic pain.�Spine�2002;27:1102-9.�[PubMed]
4.�Vroomen PCAJ, Krom MCTFM de, Knottnerus JA. Diagnostic value of history and physical examination in patients suspected of sciatica due to disc herniation: a systematic review.�J Neurol1999;246:899-906.�[PubMed]
5.�Deville WLJM, Windt DAWM, van der Dzaferagic A, Bezemer PD, Bouter LM. The test of Lasegue: systematic review of the accuracy in diagnosing herniated discs.�Spine�2000;25:1140-7.�[PubMed]
6.�Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain.�N Engl J Med�1994;331:69-73.[PubMed]
7.�Modic MT, Ross JS, Obuchowski NA, Browning KH, Cianflocco AJ, Mazanec DJ. Contrast-enhanced MR imaging in acute lumbar radiculopathy: a pilot study of the natural history.�Radiology�1995;195:429-35.�[PubMed]
8.�Modic MT, Obuchowski NA, Ross J, Brant-Zawadzki MN, Grooff PN, Mazanec DJ, et al. Acute low back pain and radiculopathy: MR imaging findings and their prognostic role and effect on outcome.�Radiology�2005;237:597-604.�[PubMed]
9.�Govind J. Lumbar radicular pain.�Aus Fam Phys�2004;33:409-12.�[PubMed]
10.�Awad JN, Moskovich R. Lumbar disc herniations: surgical versus nonsurgical treatment.�Clin Orthop Relat Res�2006;443:183-97.�[PubMed]
11.�Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with emphasis on imaging.�Ann Intern Med�2002. 137:586-97.�[PubMed]
12.�Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double blind placebo-controlled trial of evaluating the effect of piroxicam (NSAID).�Spine�1993;18:1433-8.[PubMed]
13.�Vroomen PCAJ, Krom MCTFM de, Slofstra PD, Knottnerus JA. Conservative treatment of sciatica: a systematic review.�J Spinal Dis�2000;13:463-9.�[PubMed]
14.�Luijsterburg PAJ, Verhagen AP, Ostelo RWJG, Os TAG van, Peul WC, Koes BW. Effectiveness of conservative treatments for the lumbosacral radicular syndrome: a systematic review.�Eur Spine J�2007. Apr 6;(Epub ahead of print).�[PMC free article]�[PubMed]
15.�Hagen KB, Jamtvedt G, Hilde G, Winnem MF. The updated Cochrane review of bedrest for low back pain and sciatica.�Spine�2005;30:542-6.�[PubMed]
16.�Weber H. Lumbar disc herniation. A controlled prospective study with ten years of observation.�Spine1983;8:131-40.�[PubMed]
17.�Gibson JN, Waddell G. Surgical interventions for lumbar disc prolapse.�Cochrane Database Syst Rev2007. Jan 24;(1):CD001350.�[PubMed]
18.�Van Tulder MW, Koes B, Seitsalo S, Malmivaara A. Outcome of invasive treatment modalities on back pain and sciatica: an evidence-based review.�Eur Spine J�2006;15:S82-92.�[PMC free article]�[PubMed]
19.�Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation.�Spine�2006;31:2409-14.�[PubMed]
20.�Weinstein JN, Tosteson TD, Lurie JD, Tosteson ANA, Hanscom B, Skinner JS, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT): a randomized trial.�JAMA�2006;296:2441-50.�[PMC free article]�[PubMed]
21.�Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson ANA, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT) observational cohort.�JAMA�2006;296:2451-9.�[PMC free article]�[PubMed]
22.�Koes BW, Tulder MW van, Ostelo R, Burton AK, Waddell G. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine�2001;26:2504-13.�[PubMed]
23.�Mulleman D, Mammou S, Griffoul I, Watier H, Goupille P. Pathophysiology of disc-related sciatica. I. Evidence supporting a chemical component.�Joint Bone Spine�2006;73:151-8.�[PubMed]
24.�Mulleman D, Mammou S, Griffoul I, Watier H, Goupille P. Pathophysiology of disc-related low back pain and sciatica. II. Evidence supporting treatment with TNF-alfa antagonists.�Joint Bone Spine2006;73:270-7.�[PubMed]
25.�Korhonen T, Karppinen J, Paimela L, Malmivaara A, Lindgren KA, Bowman C, et al. The treatment of disc herniation-induced sciatica with infliximab: one-year follow-up results of FIRST II, a randomized controlled trial.�Spine�2006;31:2759-66.�[PubMed]
The purpose of this article is to provide an update of a previously published evidence-based practice guideline on chiropractic management of low back pain.
Methods
This project updated and combined 3 previous guidelines. A systematic review of articles published between October 2009 through February 2014 was conducted to update the literature published since the previous Council on Chiropractic Guidelines and Practice Parameters (CCGPP) guideline was developed. Articles with new relevant information were summarized and provided to the Delphi panel as background information along with the previous CCGPP guidelines. Delphi panelists who served on previous consensus projects and represented a broad sampling of jurisdictions and practice experience related to low back pain management were invited to participate. Thirty-seven panelists participated; 33 were doctors of chiropractic (DCs). In addition, public comment was sought by posting the consensus statements on the CCGPP Web site. The RAND-UCLA methodology was used to reach formal consensus.
Results
Consensus was reached after 1 round of revisions, with an additional round conducted to reach consensus on the changes that resulted from the public comment period. Most recommendations made in the original guidelines were unchanged after going through the consensus process.
Conclusions
The evidence supports that doctors of chiropractic are well suited to diagnose, treat, co-manage, and manage the treatment of patients with low back pain disorders.
Key Indexing Terms:
Chiropractic, Low Back Pain, Manipulation, Spinal, Guidelines
Early development of the chiropractic profession in the 1900s represented the application of accumulated wisdom and traditional practices.1, 2 As was the practice of medicine, philosophy and practice of chiropractic were informed to a large extent by an apprenticeship and clinical experiential model in a time predominantly absent of clinical trials and observational research.
The traditional chiropractic approach, in which a trial of natural and less invasive methods precedes aggressive therapies, has gained credibility. However, the chiropractic profession can gain wider acceptance in the role as the first point of contact health care provider to patients with low back disorders, particularly within integrated health care delivery systems, by embracing the scientific approach integral to evidence-based health care.3, 4, 5,6, 7 It is in this context that these guidelines were developed and are updated and revised.8, 9, 10, 11, 12
By today’s standards, it is the responsibility of a health profession to use scientific methods to conduct research and critically evaluate the evidence base for clinical methods used.13, 14 This scientific approach helps to ensure that best practices are emphasized.15 With respect to low back disorders, clinical experience suggests that some patients respond to different treatments. The availability of other clinical methods for conditions that are unresponsive to more evidence-informed approaches (primary nonresponders) introduces the opportunity for patients to achieve improved outcomes by alternative and personalized approaches that may be more attuned to individual differences that cannot be informed by typical clinical trials.16, 17, 18 To a large degree, variability in the selection of treatment methods among doctors of chiropractic (DCs) continues to exist, even though the large body of research on low back pain (LBP) has focused on the most commonly used manipulative methods.17, 19, 20
Although the weight of the evidence may favor the evidence referenced in a guideline for particular clinical methods, an individual patient may be best served in subsequent trials of care by treatment that is highly personalized to their own mechanical disorder, experience of pain and disability, as well as preference for a specific treatment approach. This is consistent with the 3 components of evidence-based practice: clinician experience and judgment, patient preferences and values, and the best available scientific evidence.3, 13
Doctors of chiropractic use methods that assist patients in self-management such as exercise, diet, and lifestyle modification to improve outcomes and their stabilization to avoid dependency on health care system resources.19, 21 They also recognize that a variety of health care providers play a critical role in the treatment and recovery process of patients at various stages, and that DCs should consult, refer patients, and co-manage patients with them when in the patient’s best interest.19
To facilitate best practices specific to the chiropractic management of patients with common, primarily musculoskeletal disorders, the profession established the Council on Chiropractic Guidelines and Practice Parameters (CCGPP) in 1995.6 The organization sponsored and/or participated in the development of a number of “best practices” recommendations on various conditions.21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32 With respect to chiropractic management of LBP, a CCGPP team produced a literature synthesis8 which formed the basis of the first iteration of this guideline in 2008.9 In 2010, a new guideline focused on chronic spine-related pain was published,12 with a companion publication to both the 2008 and 2010 guidelines published in 2012, providing algorithms for chiropractic management of both acute and chronic pain.10 Guidelines should be updated regularly.33, 34 Therefore, this article provides the clinical practice guideline (CPG) based on an updated systematic literature review and extensive and robust consensus process.9, 10, 11, 12
Methods
This project was a guideline update based on current evidence and consensus of a multidisciplinary panel of experts in the conservative management of LBP. It has been recommended that, although periodic updates of guidelines are necessary, “partial updating often makes more sense than updating the whole CPG because topics and recommendations differ in terms of the need for updating.”33 Logan University Institutional Review Board determined that the project was exempt. We used Appraisal of Guidelines for Research & Evaluation (AGREE) in developing the guideline methodology.
Systematic Review
Between March 2014 through July 2014, we conducted a systematic review to update the literature published since the previous CCGPP guideline was developed. The search included articles that were published between October 2009 through February 2014. Our question was, “What is the effectiveness of chiropractic care including spinal manipulation for nonspecific low back pain?” Table 1 summarizes the eligibility criteria for the search.
Table 1
Eligibility Criteria for the Literature Search
Inclusion
Exclusion
Published between October 2009-February 2014
Case reports and case series
English language
Commentaries
Human participants
Conference proceedings
Age >17 y
In-patients
Manipulation
Letters
LBP
Narrative and qualitative reviews
Duration chronic (>3 mo)
Non–peer-reviewed publications
Patient outcomes reported
Pilot studies
Non-manipulation comparison group
Pregnancy-related LBP
RCTs, cohort studies, systematic reviews, and meta-analyses
Secondary analyses and descriptive studies
LBP, low back pain; RCT, randomized controlled trial.
Search Strategy
The following databases were included in the search: PubMed, Index to Chiropractic Literature, CINAHL, and MANTIS. Details of the strategy for each database are provided in Figure 1. Articles and abstracts were screened independently by 2 reviewers. Data were not further extracted.
Fig 1
Search strategies used in the literature search.
Evaluation of Articles
We evaluated articles using the Scottish Intercollegiate Guideline Network checklists (www.sign.ac.uk/methodology/checklists.html) for randomized controlled trials (RCTs) and systematic reviews/meta-analyses. For guidelines, the AGREE 2013 instrument35 was used. At least 2 of the 3 investigators conducting the review (CH, SW, MK) reviewed each article. If both reviewers rated the study as either high quality or acceptable, it was included for consideration; if both reviewers rated it as unacceptable, it was removed. For AGREE, we considered “unacceptable” to be a sum of <4. If there was disagreement between reviewers, a third also reviewed the article, and the majority rating was used.
Results of Literature Review
This search yielded 270 articles. Screening the articles for eligibility resulted in 18 articles included for evaluation, as detailed in Figure 2, using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.36
Fig 2
Flow diagram for literature search. LBP, low back pain; RCT, randomized controlled trial; SR, systematic reviews.
Of the 18 articles included after screening, 16 were retained as acceptable/high quality12, 17, 37, 38, 39, 40, 41, 42,43, 44, 45, 46, 47, 48, 49, 50 and 251, 52 (both systematic reviews) were excluded as being of unacceptable quality according to the Scottish Intercollegiate Guideline Network checklist. Those with new relevant information were summarized and provided to the Delphi panel as background information. Table 2 lists the articles by lead author and date, and the topic addressed, if new findings were present.
Table 2
Articles Evaluated
Lead Author
Year
Relevant New Findings
Guidelines and systematic reviews
Clar17
2014
None
Dagenais38
2010
Standards for assessment of LBP
Dagenais37
2010
Standards for assessment of LBP
Farabaugh12
2010
Basis for current update
Furlan39
2010
None
Goertz40
2012
None
Hidalgo41
2014
None
Koes42
2010
None
McIntosh43
2011
None
Posadzki44
2011
None
Rubinstein45
2013
None
Rubinstein46
2011
Excluded as unacceptable quality
Ernst51
2012
Menke52
2014
RCTs
Haas47
2013
Dosage information
Senna48
2011
Dosage information
Von Heymann49
2013
None
Walker50
2013
None
LBP, low back pain; RCT, randomized controlled trial.
Seed Documents & Seed Statements
Along with the literature summary, seed documents were comprised of the 3 previous CCGPP guidelines9, 10, 12; links were provided to full text versions. The original guidelines had been developed based on the evidence, including guidelines and research available at the time.16, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63 The steering committee, composed of authors on these previous guidelines, developed 51 seed statements based on the background documents, revising the previous statements if it seemed advisable based on the literature. The steering committee did not conduct a formal consensus process; however, the seed statement development was a team effort, with changes only made if all members of the steering committee were in agreement. Before conducting this project, these seed statements had gone through a local Delphi process among clinical and academic faculty at Logan University as part of their development of care pathways for their clinical faculty. This was done to assess the readability of the seed statements to a group of practicing clinicians. In the Delphi process, 7 statements were slightly modified from the original, and none of those changes were substantive, but rather for purposes of clarification. Consensus was reached for the seed document, which was then adopted by that institution for use in its teaching clinics. That document formed the seed document for the current project. For the Delphi rounds, the 51 statements were divided into 3 sections to be less onerous for the panelists to rate in a timely manner.
Delphi Panel
Panelists who served on the 3 previous consensus projects10, 11, 12 related to LBP management were invited to participate. Steering committee members made additional recommendations for experts in management of LBP who were not DCs to increase multidisciplinary input. There were 37 panelists; 33 were DCs, one of whom had dual licensure—DC and massage therapist. The 4 non-DC panelists consisted of an acupuncturist who is also a medical doctor, a medical doctor (orthopedic surgeon), a massage therapist, and a physical therapist. Thirty-three of the 37 panelists were in practice (89%); the mean number of years in practice was 27. Seventeen were also affiliated with a chiropractic institution (46%), with 2 of these associated with Logan University; 3 were affiliated with a different health care professional institution (8%); and 1 was employed with a government agency. Because this guideline focuses primarily on chiropractic practice in the United States, geographically, all panelists were from the United States, with 19 states represented. These were Arizona (1), California (4), Florida (3), Georgia (3), Hawaii (2), Iowa (2), Illinois (3), Kansas (1), Michigan (1), Minnesota (1), Missouri (3), North Carolina (1), New Jersey (2), New York (5), South Carolina (1), South Dakota (1), Texas (1), Virginia (1), and Vermont (1). Of the 33 DCs, 21 (64%) were members of the American Chiropractic Association, 2 (6%) were members of the International Chiropractors Association, and 10 (30%) did not belong to any national chiropractic professional organization.
Delphi Rounds and Rating System
The consensus process was conducted by e-mail. For purposes of analyzing the ratings and comments, panelists were identified by an ID number only. The Delphi panelists were not aware of other panelists’ identity during the duration of the study. As in our previous projects, we used the RAND-UCLA methodology for formal consensus.64
This methodology uses an ordinal scale of 1-9 (highly inappropriate to highly appropriate) to rate each seed statement. RAND/UCLA defines appropriateness to mean that expected patient health benefits are greater than expected negative effects by a large enough margin that the action is worthwhile, without considering costs.64
After scoring each Delphi round, the project coordinator provided the medians, percentages, and comments (as a Word table) to the steering committee. They reviewed all comments and revised any statements not reaching consensus as per these comments. The project coordinator circulated the revised statements, accompanied by the deidentified comments, to the Delphi panel for the next round.
We considered consensus on a statement’s appropriateness to have been reached if both the median rating was 7 or higher and at least 80% of panelists’ ratings for that statement were 7 or higher. Panelists were provided with space to make unlimited comments on each statement. If consensus could not be reached, it was planned that minority reports would be included.
Public Comments
As per recommendations for guideline development such as AGREE, we invited public comment on the draft CPG. This was accomplished by posting the consensus statement on the CCGPP Web site. Press releases and direct e-mail contacts announced a 2-week public comment period, with comments collected via an online Web survey application. Organizations and institutions who were contacted included the following: all US chiropractic colleges; members of all chiropractic state organizations; state boards of chiropractic examiners; chiropractic practice consultants; chiropractic attorneys; chiropractic media (including 1 publication sent to all US-licensed DCs); and chiropractic vendors, whose contacts also included interested laypersons. The steering committee then crafted additional or revised statements as per the comments collected through this method, and these statements were then recirculated through the Delphi panel until consensus was reached.
Data Analysis
For scoring purposes, ratings of 1-3 were collapsed as “inappropriate,” 4-6 as “uncertain,” and 7-9 as “appropriate.” If a panelist rated a statement as “inappropriate,” he or she was instructed to articulate a specific reason and provide a citation from the peer-reviewed literature to support it, if possible. The project coordinator entered ratings into a database (SPSS v. 22.0, Armonk, NY: IBM Corp, 2013).
Results
The verbatim evidence-informed consensus-based seed statements, as approved by the Delphi panel, are presented below. Consensus was reached after 1 round of revisions, with an additional round conducted to reach consensus on the changes that resulted from the public comment period. No minority reports are included because consensus was reached on all statements. There were 7 comments received, 6 from DCs and 1 from a layperson. Three did not require a response; statements were added or modified in response to the other 4 comments.
General Considerations
Most acute pain, typically the result of injury (micro- or macrotrauma), responds to a short course of conservative treatment (Table 3). If effectively treated at this stage, patients often recover with full resolution of pain and function, although recurrences are common. Delayed or inadequate early clinical management may result in increased risk of chronicity and disability. Furthermore, those responding poorly in the acute stage and those with increased risk factors for chronicity must also be identified as early as possible.
Table 3
Frequency and Duration for Trial(s) of Chiropractic Treatment
Scheduled ongoing care for management of chronic painb
1-4 visits per month
At minimum every 6 visits, or as necessary to document condition changes.
aFor acute and subacute stages; up to 12 visits per trial of care. If additional trials of care are indicated, supporting documentation should be available for review, including, but not necessarily limited to, documentation of complicating factors and/or comorbidities coupled with evidence of functional gains from earlier trial(s). Efforts toward self-care recommendations should be documented.
bFor chronic presentations, exacerbations, and scheduled ongoing care for management of chronic pain, additional care must be supported with evidence of either functional improvement or functional optimization. Such presentations may include, but are not limited to, the following: (1) substantial symptom recurrences following treatment withdrawal, (2) minimization/control of pain, (3) maintenance of function and ability to perform common ADLs, (4) minimization of dependence on therapeutic interventions with greater risk(s) of adverse events, and (5) care which maintains or improves capacity to perform work. Efforts toward self-care recommendations should be documented.
Clinicians must continually be vigilant for the appearance of clinical red flags that may arise at any point during patient care. In addition, biopsychosocial factors (also known as clinical yellow flags) should be identified and addressed as early as possible as part of a comprehensive approach to clinical management.
Chiropractic doctors are skilled in multiple approaches of functional assessment and treatment. Depending on the clinical complexity, DCs can work independently or as part of a multidisciplinary team approach to functional restoration of patients with acute and chronic LBP.
It is the ultimate goal of chiropractic care to improve patients’ functional capacity and educate them to accept independently the responsibility for their own health.
Informed Consent
Informed consent is the process of proactive communication between a patient and physician that results in the patient’s authorization or agreement to undergo a specific medical intervention. Informed consent should be obtained from the patient and performed within the local and/or regional standards of practice. The DC should explain the diagnosis, examination, and proposed procedures clearly and simply and answer patients’ questions to ensure that they can make an informed decision about their health care choices. He or she should explain material risks* of care along with other reasonable treatment options, including the risks of no treatment. (*Note: The legal definition of material risk may vary state by state.)
Examination Procedures
Thorough history and evidence-informed examination procedures are critical components of chiropractic clinical management. These procedures provide the clinical rationale for appropriate diagnosis and subsequent treatment planning.
Assessment should include but is not limited to the following38:
Health history (eg, pain characteristics, red flags, review of systems, risk factors for chronicity)
Specific causes of LBP (eg, aortic aneurysm, inflammatory disorders)
Diagnostic testing (indications) for red flags (eg, imaging and laboratory tests)
Routine imaging or other diagnostic tests are not recommended for patients with nonspecific LBP.55
Imaging and other diagnostic tests are indicated in the presence of severe and/or progressive neurologic deficits or if the history and physical examination cause suspicion of serious underlying pathology.55
Patients with persistent LBP accompanied by signs or symptoms of radiculopathy or spinal stenosis should be evaluated, preferably, with magnetic resonance imaging or computed tomography.55
Imaging studies should be considered when patients fail to improve following a reasonable course of conservative care or when there is suspicion of an underlying anatomical anomaly, such as spondylolisthesis, moderate to severe spondylosis, posttrauma with worsening symptomatogy (consider imaging, referral, or co-management) with evidence of persistent or increasing neurological (ie, reflex, motor, and/or sensory) compromise, or other factors which might alter the treatment approach. Lateral view flexion/extension studies may be warranted to assess for mechanical instability due to excessive intervertebral translation and/or wedging. Imaging studies should be considered only after careful review and correlation of the history and examination.65
Severity and Duration of Conditions
Conditions of illness and injury are typically classified by severity and/or duration. Common descriptions of the stages of illness and injuries are acute, subacute, chronic, and recurrent, and further subdivided into mild, moderate, and severe.
Acute—symptoms persisting for less than 6 weeks.
Subacute—symptoms persisting between 6 and 12 weeks.
Chronic—symptoms persisting for at least 12 weeks’ duration.
Recurrent/flare-up—return of symptoms perceived to be similar to those of the original injury at sporadic intervals or as a result of exacerbating factors.
Treatment Frequency and Duration
Although most patients respond within anticipated time frames, frequency and duration of treatment may be influenced by individual patient factors or characteristics that present as barriers to recovery (eg, comorbidities, clinical yellow flags). Depending on these individualized factors, additional time and treatment may be required to observe a therapeutic response. The therapeutic effects of chiropractic care/treatment should be evaluated by subjective and/or objective assessments after each course of treatment (see “Outcome Measurement”).
Recommended therapeutic trial ranges are representative of typical care parameters. A typical initial therapeutic trial of chiropractic care consists of 6 to 12 visits over a 2- to 4-week period, with the doctor monitoring the patient’s progress with each visit to ensure that acceptable clinical gains are realized (Table 3).
For acute conditions, fewer treatments may be necessary to observe a therapeutic effect and to obtain complete recovery. Chiropractic management is also recommended for various chronic low back conditions where repeated episodes (or acute exacerbations) are experienced by the patient, particularly when a previous course of care has demonstrated clinical effectiveness and reduced the long-term use of medications.
Initial Course of Treatments for Low Back Disorders
To be consistent with an evidence-based approach, DCs should use clinical methods that generally reflect the best available evidence, combined with clinical judgment, experience, and patient preference. For example, currently, the most robust literature regarding manual therapy for LBP is based primarily on high-velocity, low-amplitude (HVLA) techniques, and mobilization (such as flexion-distraction).17, 20, 66 Therefore, in the absence of contraindications, these methods are generally recommended. However, best practices for individualized patient care, based on clinical judgment and patient preference, may require alternative clinical strategies for which the evidence of effectiveness may be less robust.
The treatment recommendations that follow, based on clinical experience combined with the best available evidence, are posited for the “typical” patient and do not include risk stratification for complicating factors. Complicating factors are discussed elsewhere in this document.
An initial course of chiropractic treatment typically includes 1 or more “passive” (ie, nonexercise) manual therapeutic procedures (ie, spinal manipulation or mobilization) and physiotherapeutic modalities for pain reduction, in addition to patient education designed to reassure and instill optimal strategies for independent management.
Although the evidence reviewed does not generally support the use of therapeutic modalities (ie, ultrasonography, electrical stimulation, etc) in isolation,67 their use as part of a passive-to-active care multimodal approach to LBP management may be warranted based on clinician judgment and patient preferences. Because of the scarcity of definitive evidence,68 lumbar supports (bracing/taping/orthoses) are not recommended for routine use, but there may be some utility in both acute and chronic conditions based upon clinician judgment, patient presentation, and preferences. Caution should be exercised as these orthopedic devices may interfere with conditioning and return to regular activities of daily living (ADLs).
The initial visits allow the doctor to explain that the clinician and the patient must work as a proactive team and to outline the patient’s responsibilities. Although passive care methods for pain or discomfort may be initially emphasized, “active” (ie, exercise) care should be increasingly integrated to increase function and return the patient to regular activities. Table 3 lists appropriate frequency and duration ranges for trials of chiropractic treatment for different stages of LBP.
Reevaluation & Reexamination
After an initial course of treatment has been concluded, a detailed or focused reevaluation should be performed. The purpose of this reevaluation is to determine whether the patient has made clinically meaningful improvement. A determination of the necessity for additional treatment should be based on the response to the initial trial of care and the likelihood that additional gains can be achieved.
As patients begin to plateau in their response to treatment, further care should be tapered or discontinued depending on the presentation. A reevaluation is recommended to confirm that the condition has reached a clinical plateau or has resolved. When a patient reaches complete or partial resolution of their condition and all reasonable treatment and diagnostic studies have been provided, then this should be considered a final plateau (maximum therapeutic benefit, MTB). The DC should perform a final examination, typically following a trial of therapeutic withdrawal, to verify that MTB has been achieved and provide any necessary patient education and instructions in effective future self-management and/or the possible need for future chiropractic care to retain the benefits achieved.
Continuing Course Of Treatment
If the criteria to support continuing chiropractic care (substantive, measurable functional gains with remaining functional deficits) have been achieved, a follow-up course of treatment may be indicated. However, one of the goals of any treatment plan should be to reduce the frequency of treatments to the point where MTB continues to be achieved while encouraging more active self-therapy, such as independent strengthening and range of motion exercises and rehabilitative exercises. Patients also need to be encouraged to return to usual activity levels as well as to avoid catastrophizing and overdependence on physicians, including DCs. The frequency of continued treatment generally depends on the severity and duration of the condition. Patients who are interested in wellness care (formerly called maintenance care11) should be given those options as well. (Wellness or maintenance care was defined by Dehen et al11 as “care to reduce the incidence or prevalence of illness, impairment, and risk factors and to promote optimal function.”)
When the patient’s condition reaches a plateau or no longer shows ongoing improvement from the therapy, a decision must be made on whether the patient will need to continue treatment. Generally, progressively longer trials of therapeutic withdrawal may be useful in ascertaining whether therapeutic gains can be maintained without treatment.
In a case where a patient reaches a clinical plateau in their recovery (MTB) and has been provided reasonable trials of interdisciplinary treatments, additional chiropractic care may be indicated in cases of exacerbation/flare-up or when withdrawal of care results in substantial, measurable decline in functional or work status. Additional chiropractic care may be indicated in cases of exacerbation/flare-up in patients who have previously reached MTB if criteria to support such care (substantive, measurable prior functional gains with recurrence of functional deficits) have been established.
Outcome Measurement
For a trial of care to be considered beneficial, it must be substantive, meaning that a definite improvement in the patient’s functional capacity has occurred. Examples of measurable outcomes and activities of daily living and employment include the following:
1.Pain scales such as the visual analog scale and the numeric rating scale.
2.Pain diagrams that allow the patient to demonstrate the location and character of their symptoms.
3.Validated ADL measures, such as the Revised Oswestry Back Disability Index, Roland Morris Back Disability Index, RAND 36, and Bournemouth Disability Questionnaire.
4.Increases in home and leisure activities, in addition to increases in exercise capacity.
5.Increases in work capacity or decreases in prior work restrictions.
6.Improvement in validated functional capacity testing, such as lifting capacity, strength, flexibility, and endurance.
Spinal Range Of Motion Assessment
Range of motion testing may be used as a part of the physical examination to assess for regional mobility, although evidence does not support its reliability in determining functional status.69
Benefit Vs Risk
Care rendered by DCs has been documented to be quite safe and effective compared with other common medical treatments and procedures. A 2010 systematic review concluded that serious adverse events were no more than 1 per million patient visits for lumbar spine manipulation.20 Another systematic review found that the risk of major adverse events with manual therapy is low, but many patients experience minor to moderate short-lived (<48 hours) adverse events after treatment.70
These are usually brief episodes of muscle stiffness or soreness.20 The relative risk (RR) of adverse events appears greater with drug therapy but less with usual medical care.70 Comparatively, an earlier study from 1995 related to cervical manipulation found that the RR for high-velocity manipulation causing minor/moderate adverse events was significantly less than the RR of the comparison medication (usually nonsteroidal anti-inflammatory drugs [NSAIDs]).71 The risk of death from NSAIDs for osteoarthritis was estimated to be 100-400 times the risk of death from cervical manipulation.71 Because lumbar spine manipulation is considered lower risk than cervical manipulation, it is reasonable to extrapolate that NSAIDs pose at least the same comparative risk when prescribed for the treatment of LBP. Special attention must be given to each patient’s individual history and presentation. In that context, it should be noted that for patients who are not good candidates for HVLA manipulation, DCs should modify their manual approach accordingly.
Cautions & Contraindications
Chiropractic-directed care, including patient education, and passive and active care therapy, is a safe and effective form of health care for low back disorders. As stated in the previous section, there are certain clinical situations where HVLA manipulation or other manual therapies may be contraindicated. It is incumbent upon the treating DC to evaluate the need for care and the risks associated with any treatment to be applied. Many contraindications are considered relative to the location and stage of severity of the morbidity, whether there is co-management with one or more specialists, and the therapeutic methods being used by the chiropractic physician. Figure 3 lists contraindications for high-velocity manipulation to the lumbar spine (red flags); however, these do not necessarily prohibit soft-tissue, low-velocity, low-amplitude procedures and mobilization.
Fig 3
Contraindications for high-velocity manipulation to the lumbar spine (red flags). aIn some cases, soft-tissue, low-velocity, low-amplitude mobilization procedures may still be clinically reasonable and safe.
Conditions Contraindicating Certain Chiropractic-Directed Treatments Such As Spinal Manipulation & Passive Therapy
In some complex cases where biomechanical, neurological, or vascular structure or integrity is compromised, the clinician may need to modify or omit the delivery of manipulative procedures. Chiropractic co-management may still be appropriate using a variety of treatments and therapies commonly used by DCs. It is prudent to document the steps taken to minimize the additional risk that these conditions may present. Figure 4 lists conditions which present contraindications to spinal manipulation and passive therapy, along with conditions requiring co-management and/or referral.
Fig 4
Conditions contraindicating certain chiropractic-directed treatments such as spinal manipulation and passive therapy.
During the course of ongoing chronic pain management of spine-related conditions, the provider must remain alert to the emergence of well-known and established “red flags” that could indicate the presence of serious pathology. Patients presenting with “red flag” signs and/or symptoms require prompt diagnostic workup which can include imaging, laboratory studies, and/or referral to another provider. Ignoring these “red flag” indicators increases the likelihood of patient harm. Figure 5 summarizes red flags that present contraindications to ongoing HVLA spinal manipulation.
Fig 5
Complicating factors that may document the necessity of ongoing care for chronic conditions.
Management of Chronic LBP
Definition of chronic pain patients. Note: MTB is defined as the point at which a patient’s condition has plateaued and is unlikely to improve further. Chronic pain patients are those for whom ongoing supervised treatment/care has demonstrated clinically meaningful improvement with a course of management and who have reached MTB, but in whom substantial residual deficits in activity performance remain or recur upon withdrawal of treatment. The management for chronic pain patients ranges from home-directed self-care to episodic care to scheduled ongoing care. Patients who require provider-assisted ongoing care are those for whom self-care measures, although necessary, are not sufficient to sustain previously achieved therapeutic gains; these patients may be expected to progressively deteriorate as demonstrated by previous treatment withdrawals.
Chronic Care Goals
Minimize lost time on the job
Support patient’s current level of function/ADL
Pain control/relief to tolerance
Minimize further disability
Minimize exacerbation frequency and severity
Maximize patient satisfaction
Reduce and/or minimize reliance on medication
Application of Chronic Pain Management
Chronic pain management occurs after the appropriate application of active and passive care including lifestyle modifications. It may be appropriate when rehabilitative and/or functional restorative and other care options, such as psychosocial issues, home-based self-care, and lifestyle modifications, have been considered and/or attempted, yet treatment fails to sustain prior therapeutic gains and withdrawal/reduction results in the exacerbation of the patient’s condition and/or adversely affects their ADLs.
Ongoing care may be inappropriate when it interferes with other appropriate care or when the risk of supportive care outweighs its benefits, that is, physician dependence, somatization, illness behavior, or secondary gain. However, when the benefits outweigh the risks, ongoing care may be both medically necessary and appropriate.
Appropriate chronic pain management of spine-related conditions includes addressing the issues of physician dependence, somatization, illness behavior, and secondary gain. Those conditions that require ongoing supervised treatment after having first achieved MTB should have appropriate documentation that clearly describes them as persistent or recurrent conditions. Once documented as persistent or recurrent, these chronic presentations should not be categorized as “acute” or uncomplicated.
Factors Affecting the Necessity for Chronic Pain Management of LBP
Prognostic factors that may provide a partial basis for the necessity for chronic pain management of LBP after MTB has been achieved include the following:
Older age (pain and disability)
History of prior episodes (pain, activity limitation, disability)
Duration of current episode >1 month (activity limitation, disability)
Leg pain (for patients having LBP) (pain, activity limitation, disability)
Psychosocial factors (depression [pain]; high fear-avoidance beliefs, poor coping skills [activity limitation]; expectations of recovery)
High pain intensity (activity limitation; disability)
Occupational factors (higher job physical or psychological demands [disability])
The list above is not all-inclusive and is provided to represent prognostic factors most commonly seen in the literature. Other factors or comorbidities not listed above may adversely affect a given patient’s prognosis and management. These should be documented in the clinical record and considered on a case-by-case basis.
Each of the following factors may complicate the patient’s condition, extend recovery time, and result in the necessity of ongoing care:
Nature of employment/work activities or ergonomics: The nature and psychosocial aspects of a patient’s employment must be considered when evaluating the need for ongoing care (eg, prolonged standing posture, high loads, and extended muscle activity)
Impairment/disability: The patient who has reached MTB but has failed to reach preinjury status has an impairment/disability even if the injured patient has not yet received a permanent impairment/disability award.
Medical history: Concurrent condition(s) and/or use of certain medications may affect outcomes.
History of prior treatment: Initial and subsequent care (type and duration), as well as patient compliance and response to care, can assist the physician in developing appropriate treatment planning. Delays in the initiation of appropriate care may complicate the patient’s condition and extend recovery time.
Lifestyle habits: Lifestyle habits may impact the magnitude of treatment response, including outcomes at MTB.
Psychological factors: A history of depression, anxiety, somatoform disorder, or other psychopathology may complicate treatment and/or recovery.
Treatment Withdrawal Fails to Sustain MTB
Documented flare-ups/exacerbations (ie, increased pain and/or associated symptoms, which may or may not be related to specific incidents), superimposed on a recurrent or chronic course, may be an indication of chronicity and/or need for ongoing care.
Complicating/Risk Factors for Failure to Sustain MTB
Figure 5 lists complicating factors that may document the necessity of ongoing care for chronic spine-related conditions. Such lists of complicating/risk factors are not all-inclusive. Individual factors from this list may adequately explain the condition chronicity, complexity, and instability in some cases. However, most chronic cases that require ongoing care are characterized by multiple complicating factors. These factors should be carefully identified and documented in the patient’s file to support the characterization of a condition as chronic.
Risk Factors for the Transition of Acute/Subacute Spine-Related Conditions to Chronicity (Yellow Flags)
A number of prognostic variables have been identified as increasing the risk of transition from acute/subacute to chronic nonspecific spine-related pain. However, their independent prognostic value is low. A multidimensional model, that is, a number of clinical, demographic, psychological, and social factors are considered simultaneously, has been recommended. This model emphasizes the interaction among these factors, as well as the possible overlap between variables such as pain beliefs and pain behaviors.
Chronicity may be described in terms of pain and/or activity limitation (function) and/or work disability. Risk factors for chronicity have been categorized by similar domains:
Symptoms
Psychosocial factors
Function
Occupational factors
Factors directly associated with the clinician/patient encounter may influence the transition to chronicity:
Treatment expectations: Patients with high expectations for a specific treatment may contribute to better functional outcomes if they receive that treatment.
Significant others’ support: Patients’ risk of chronicity may be reduced when family members encourage their participation in social and recreational activities.
Diagnosis Of Chronic LBP
The diagnosis should never be used exclusively to determine need for care (or lack thereof). The diagnosis must be considered with the remainder of case documentation to assist the physician or reviewer in developing a comprehensive clinical picture of the condition/patient under treatment.
Clinical Reevaluation Information
Clinical information obtained during reevaluation that may be used to document the necessity of chronic pain management for persistent or recurrent spine-related conditions includes, but is not limited to, the following:
Response to date of care management for the current and previous episodes.
Response to therapeutic withdrawal (either gradual or complete withdrawal) or absence of care.
MTB has been reached and documented.
Patient-centered outcome assessment instruments.
Analgesic use patterns.
Other health care services used.
Clinical Reevaluation Information to Document Necessity for Ongoing Care of Chronic LBP
In addition to standard documentation elements (ie, date, history, physical evaluation, diagnosis, and treatment plan), the clinical information typically relied upon to document the necessity of ongoing chronic pain management includes the following:
Documentation of having achieved a clinically meaningful favorable response to initial treatment or documentation that the plan of care is to be amended.
Documentation that the patient has reached MTB.
Substantial residual deficits in activity limitations are present at MTB.
Documented attempts of transition to primary self-care.
Documented attempts and/or consideration of alternative treatment approaches.
Documentation of those factors influencing the likelihood that self-care alone will be insufficient to sustain or restore MTB.
Once the need for additional care has been documented, findings of diagnostic/assessment procedures that may influence treatment selection include the following:
Biomechanical analysis (pain, asymmetry, range of motion, tissue tone changes);
Palpation (static, motion);
Nutritional/dietary assessment with respect to factors related to pain management (such as vitamin D intake).
This list is provided for guidance only and is not all-inclusive. All items are not required to justify the need for ongoing care. Each item of clinical information should be documented in the case file to describe the patient’s clinical status, present and past.
In the absence of documented flare-up/exacerbation, the ongoing treatment of persistent or recurrent spine-related disorders is not expected to result in any clinically meaningful change. In the event of a flare-up or exacerbation, a patient may require additional supervised treatment to facilitate return to MTB status. Individual circumstances including patient preferences and previous response to specific interventions guide the appropriate services to be used in each case.
Chronic Pain Management Components in Physician-Directed Case Management
Case management of patients with chronic LBP should be based upon an individualized approach to care that combines the best evidence with clinician judgment and patient preferences. In addition to spinal manipulation and/or mobilization, an active care plan for chronic pain management may include, but is not restricted to, the following:
Procedures
Massage therapy
Other manual therapeutic methods
Physical modalities
Acupunctur
Bracing/orthoses
Behavioral and exercise recommendations
Supervised rehabilitative/therapeutic exercise
General and/or specific exercise programs
Mind/body programs (eg, yoga, Tai Chi)
Multidisciplinary rehabilitation
Cognitive behavioral programs
Counseling recommendations
ADL recommendations
Co-management/coordination of care with other physicians/health care providers
Monitoring patient compliance with self-care recommendations
Chronic Pain Management Treatment Planning
A variety of functional and physiological changes may occur in chronic conditions. Therefore, a variety of treatment procedures, modalities, and recommendations may be applied to benefit the patient. The necessity for ongoing chronic pain management of spine-related conditions for individual patients is established when there is a return of pain and/or other symptoms and/or pain-related difficulty performing tasks and actions equivalent to the appropriate minimal clinically important change value for more than 24 hours, for example, change in numeric rating scale of more than 2 points for chronic LBP.
Although the visit frequency and duration of supervised treatment vary and are influenced by the rate of recovery toward MTB values and the individual’s ability to self-manage the recurrence of complaints, a reasonable therapeutic trial for managing patients requiring ongoing care is up to 4 visits after a therapeutic withdrawal. If reevaluation indicates further care, this may be delivered at up to 4 visits per month. (Caution: The majority of chronic pain patients can self/home-manage, be managed in short episodic bursts of care, or require ongoing care at 1-2 visits per month, to be reevaluated at a minimum of every 12 visits. It is rare that a patient would require 4 visits per month to manage even advanced or complicated chronic pain.) Clinicians should routinely monitor a patient’s change in pain/function to determine appropriateness of continued care. An appropriate reevaluation should be completed at minimum every 12 visits. Reevaluation may be indicated more frequently in the event a patient reports a substantial or unanticipated change in symptoms and/or there is a basis for determining the need for change in the treatment plan/goals.
When pain and/or ADL dysfunction exceeds the patient’s ability to self-manage, the medical necessity of care should be documented and the chronic care treatment plan altered appropriately.
Patient recovery patterns vary depending on degrees of exacerbations. Mild exacerbation episodes may be manageable with 1-6 office visits within a chronic care treatment plan. There is not a linear effect between the intensity of exacerbation and time to recovery.
Moderate and severe exacerbation episodes within a chronic care treatment plan require acute care recommendations and case management.12
Algorithms
Figure 6 summarizes the pathways for the chiropractic management of LBP.
Fig 6
Algorithms for chiropractic management of LBP.
Discussion
With the chiropractic profession’s establishment of the CCGPP to facilitate the development of best practices, 3 guidelines addressing the management of low back disorders were ultimately published.9, 10, 12 This set in motion an effort to improve clinical methods by reducing variation in chiropractic treatment patterns that has long been unaddressed by any other evidence-informed and consensus-driven official guideline.16, 54, 55, 62, 63,72 The approach to the development of these recommendations has been evolutionary so as to guide the profession toward the utilization of more evidence-informed clinical methods intended to improve patient outcomes. Historically, this also explains why the initial low back guideline, published in 2008, required 2 subsequent additional guidelines to expand on acute and chronic conditions. This was practical to introduce additional guidance in a stepwise fashion.
The focus of these recommendations has been patient centered and not practitioner centered. Practices and techniques that have not demonstrated superior efficacy in published studies may be used as alternative approaches to those methods that have more robust evidence. No other guidelines have been specific to this purpose within the chiropractic profession and endorsed as broadly, making this guideline unique. It is also important to consider that guidelines specific to other professions may or may not include clinical approaches that do not best inform chiropractic management of low back disorders. Although evidence produced under the auspices of other professions is important to consider, it is also important to consider whether this evidence informs a conservative care approach. For example, from a chiropractic viewpoint, drug and surgical treatment approaches are generally regarded as more invasive and should be considered as second- and third-line approaches to the treatment of low back disorders. That is why we believe that professional guidelines specific to a profession’s scope and approach to intervening in the natural course of disease are important.
It is the responsibility of a profession to periodically update guidelines to ensure consistency with new research findings and subsequent clinical experience. As such, an updated literature review was conducted, and the previous best practice guidelines were revised. The evidence reviewed has informed several important new recommendations to this updated guideline. For example, the evidence informs us that the routine use of radiographic imaging studies is not in the best interest of most patients with nonspecific LBP.53, 55 However, there may be exceptions to this based upon history and clinical examination characteristics. Doctors of chiropractic are advised that it is frequently in the best interest of patients to select manual method approaches that do not rely on radiographs to determine the method of manipulation or adjustment.69 In addition, it is not in the patient’s best interest for the DC to use the least evidence-informed chiropractic techniques as their first-line approach over those where the evidence is more robust.
While adding important new recommendations, it is useful to note that the updated literature synthesis did not ultimately require many other changes from the original guideline recommendations. The changes reflected in this current update were as follows: (1) a brief description of key elements that should standardly be included during an informed consent discussion; (2) the recommendation that routine radiographs, other imaging, and other diagnostic tests are not recommended for patients with nonspecific LBP (along with recommendations for when these studies should be considered); (3) recommendation that the hierarchy of clinical methods used in patient care should generally correspond to the supporting level of existing evidence; (4) additional clarification about the limited use of therapeutic modalities and lumbar supports that reflects patient preferences with the intention to best facilitate the shift from passive-to-active care and not dependency on passive modalities with limited evidence of efficacy; (5) recognition that although range of motion testing may be clinically useful as a part of the physical examination to assess for regional mobility, the evidence does not support its reliability in determining functional status; and (6) inclusion of a brief summary of the evidence informing manipulation risk vs benefit assessment.
Although this revision contemplates new guidance on key practice areas, it is not expected that these new recommendations will necessarily apply to every patient seen by a DC.
Similarly, with respect to the dosage recommendations (ie, treatment frequency and duration) within this guideline, dosage should be modified to fit the individual patient’s needs. For example, the majority of chronic pain patients can self-manage, can be managed in short episodic bursts of care, or require ongoing care at 1-2 visits per month, to be reevaluated at a minimum of every 12 visits. It is rare that a patient would require 4 visits per month to manage advanced or complicated chronic pain. Thus, it is important to consider this guideline’s recommendations for visit frequency as ranges rather than specific numbers. In addition, with regard to continuing assessments to evaluate the effectiveness of treatment, after the initial round of up to 6 visits, a brief evaluation should be performed to evaluate the progress of care. Such reevaluations at a minimum should include assessment of subjective and/or objective factors. These might include using pain scales such as the visual analog scale, the numeric rating scale, pain diagrams, and/or validated ADL measures, such as the Revised Oswestry Back Disability Index, Roland Morris Back Disability Index, RAND 36, or the Bournemouth Disability Questionnaire. Additional orthopedic/neurological tests may be considered on a case-by-case basis.
Nothing in this guideline should be interpreted as saying that patients should never have imaging ordered based upon examination and clinical judgment. Similarly, the conclusion should not be that every patient should only receive treatment methods with the highest level of evidence. It is the recommendation of this guideline that imaging and clinical methods have evidence to inform their use. In addition, patients should be informed when their care appears to require a trial of an alternate, less evidence-informed strategy.
Regarding the evidence used to support these guidelines, most clinical trials are limited in duration and usually reflect a target patient population that is not necessarily representative of all patients encountered in standard practice. Patients possess characteristics that include risk factors (ie, age, history of previous episodes of LBP, etc) and other clinical characteristics that were not specifically assessed in clinical trials. Therefore, it is important to view practice guidelines in this context and that a 1-size-fits-all approach will not fit all patients. It is the collective judgment of CCGPP, the Delphi panelists, and the authors that unexplainable and unnecessary variation in treatment patterns for standard presentations of nonspecific LBP, without considering or using the best evidence, will not necessarily lead to improvements in clinical methods and improved patient outcomes.
Future Studies
The work of developing and improving guidelines is a never-ending and time-consuming task. Therefore, the authors have suggested areas of patient management that should be considered during future revisions. Three areas suggested during the manuscript review process were (1) guidance on the evidence of the value of limited rest at various phases of recovery across the range of low back disorders, (2) more detailed guidance as to what history findings would/should lead to imaging, and (3) review of the literature describing efforts to develop assessment methods and tools to characterize the predictors of outcomes and inform selection and greater standardization of clinical methods.73, 74 Two areas of focus for future updates are also strongly recommended by the coauthors as well. The first concerns attempting to achieve a more detailed understanding of the hierarchy of chiropractic techniques that should be used based upon various archetypal patient presentations across the range of low back disorders. This would require reviewing head-to-head comparative research to determine relative efficacy of clinical methods using specific chiropractic techniques.
The authors recognize that some legacy outcome measures used in clinical practice and in clinical trials were not developed specifically with patients who may be interested in prioritizing conservative care approaches first. Also, because a measure’s ability to detect change and clinically minimal important difference (CMID) is linked directly to the target population and contextual characteristics, it is unlikely that there is a monolithic CMID value for a clinical outcomes assessment tool (including patient rated outcome measures) across all contexts of use and patient cohorts. More likely, there would be a range in CMID estimates that differs across varying patient cohorts and clinical trial contexts.75 The chiropractic profession has relied upon instruments that are less sensitive to changes in the types of risks, adverse effects, symptoms, and impacts that chiropractic patients might consider most important. This includes the benefits of avoidance of risks and adverse events associated with medication use and surgical interventions. As such, a comprehensive review is recommended to determine the evidence for the use of these legacy instruments in practice as well as, most critically, clinical trials that include the evaluation of the outcomes of the treatment of low back disorders that include chiropractic subjects. This type of review should include members who have a background in outcomes measurement and the development of de novo patient-reported outcomes instruments. Finally, an ever-broadening horizon of new and ongoing areas of related research constantly needs to be scanned for updated and applicable learnings, such as improved understanding of the interplay between functional anatomy (eg, muscular and fascial) and the generation of LBP.76, 77
Limitations
This guideline did not address several important issues that future efforts should focus on, including the following: the important issues of appropriate recommendations on limited rest; guidance on how DCs should assess history findings that might require imaging; expanded review and assessment of comparative efficacy of chiropractic manipulative techniques; and a full-scale review of outcome measures used by chiropractors and chiropractic researchers to evaluate the suitability of legacy measures as well as the robustness of their reported CMID in the context of populations frequently treated by chiropractors.78, 79, 80
Our Delphi panel may not have represented the broadest spectrum of DCs in terms of philosophy and approach to practice. In addition, this guideline is most applicable to chiropractic practice in the United States. Input from other professions was present but also limited to 4 members from other professions (acupuncture, massage therapy, medicine, and physical therapy). However, the panel had geographic diversity and was clearly based upon practice expertise with 33 of 37 panelists being in practice an average 27 years.
Another limitation relates to the literature included in the systematic review, which extended through February 2014 to provide time for project implementation. It is possible that articles were inadvertently excluded. An important issue related to the literature is that issues of great practical importance, such as the determination of optimal procedures and protocols for specific patients, do not yet have enough high-quality evidence to make detailed recommendations. An example of this is the use of a wide variety of manipulative techniques by DCs,19even though most randomized trials use only HVLA manipulation, due to the requirements of the study design for uniformity of the intervention. As the evidence base for manipulative techniques grows and expands its scope, it is essential that CPGs continue to be updated in response to new evidence. Although the authors did not task themselves with the responsibility of developing a formal dissemination plan, CCGPP is currently developing one to coordinate with the timing of the publication of this guideline.
Finally, any guideline recommendations are limited by those who would use partial statements, out of context, to justify a treatment, utilization, and/or reimbursement decision. It is critical to the appropriate use of this CPG that recommendations are not misconstrued by being taken out of context by the use of partial statements. To avoid such practice, we strongly recommend that when a quote from this guideline is to be used, an entire paragraph be included to contextualize the recommendation being cited.
Conclusion
This publication is an update of the best practice recommendations for chiropractic management of LBP.9, 10, 12This guide summarizes recommendations throughout the continuum of care from acute to chronic and offers the chiropractic profession and other key stakeholders an up-to-date evidence- and clinical practice experience–informed resource outlining best practice approaches for the treatment of patients with LBP.
Funding Sources & Conflicts of Interest
All authors and panelists participated without compensation from any organization. Logan University made an in-kind contribution to the project by allowing Drs. Hawk and Kaeser and Ms. Anderson and Walters to devote a portion of their work time to this project. The University of Western States also provided in-kind support for a portion of Dr. Hawk’s time. Dr. Farabaugh currently holds the position of the National Physical Medicine Director of Advanced Medical Integration Group, LP. Dr. Morris is a post-graduate faculty member of the National University of Health Sciences and receives access to library resources. There were no conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): C.H., G.G., C.M., W.W., G.B.
Design (planned the methods to generate the results): C.H., G.G.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): C.H., G.G., C.M.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): C.H.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): C.H., G.G., C.M., G.B.
Literature search (performed the literature search): C.H., M.K., S.W., R.F., G.G., C.M.
Writing (responsible for writing a substantive part of the manuscript): C.H., R.F., G.G., C.M., W.W., G.B.
Critical review (revised manuscript for intellectual content; this does not relate to spelling and grammar checking): C.H., M.K., S.W., R.F., M.D., G.G., C.M., W.W., M.D., G.B., T.A.
Acknowledgment
The authors thank Michelle Anderson, project coordinator, who ensured that all communications were completed smoothly and in a timely manner. The experts, listed below, who served on the Delphi panel made this project possible by generously donating their expertise and clinical judgment.
Logan University panelists who developed the seed document that served as the basis for the consensus process: Robin McCauley Bozark, DC; Karen Dishauzi, DC, MEd; Krista Gerau, DC; Edward Johnnie, DC; Aimee Jokerst, DC; Jeffrey Kamper, DC; Norman Kettner, DC; Janine Ludwinski, DC; Donna Mannello, DC; Anthony Miller, DC; Patrick Montgomery, DC; Michael J. Wittmer, DC. Muriel Perillat, DC, MS, Logan Dean of Clinics, also provided an independent review of the document.
Delphi panelists for the consensus process: Charles Blum, DC; Bryan Bond, DC; Jeff Bonsell, DC; Jerrilyn Cambron, LMT, DC, MPH, PhD; Joseph Cipriano, DC; Mark Cotney, DC; Edward Cremata, DC; Don Cross, DC; Donald Dishman, DC; Gregory Doerr, DC; Paul Dougherty, DC; Joseph Ferstl, DC; Anthony Q. Hall, DC; Michael W. Hall, DC; Robert Hayden, DC, PhD; Kathryn Hoiriis, DC; Lawrence Humberstone, DC; Norman Kettner, DC; Robert Klein, DC; Kurt Kuhn, DC, PhD; William Lauretti, DC; Gene Lewis, DC, MPH; John Lockenour, DC; James McDaniel, DC; Martha Menard, PhD, LMT; Angela Nicholas, DC; Mariangela Penna, DC; Dan Spencer, DC; Albert Stabile, DC; John S. Stites, DC; Kasey Sudkamp, DPT; Leonard Suiter, DC; John Ventura, DC; Sivarama Vinjamury, MD, MAOM, MPH, LAc; Jeffrey Weber, MA, DC; Gregory Yoshida, MD.
References
Meeker, S HW. Chiropractic: a profession at the crossroads of mainstream and alternative medicine. Ann Intern Med. 2002; 136: 216–227
Coulter, I. The roles of philosophy and belief systems in complementary and alternative health care.in: Paper presented at: Conference on Philosophy of Chiropractic Education 2000; Toronto. ; 2000
LeFebvre, R, Peterson, D, and Haas, M. Evidence-based practice and chiropractic care. JEBCAM. 2013; 18: 75–79
Triano, J and Raley, B. Chiropractic in the interdisciplinary team practice. Top Clin Chiropr. 1994; 1: 58–66
Triano, JJ. Literature syntheses for the Council on Chiropractic Guidelines and Practice Parameters: methodology. J Manipulative Physiol Ther. 2008; 31: 645–650
Triano, JJ. What constitutes evidence for best practice?. J Manipulative Physiol Ther. 2008; 31: 637–643
Triano, JJ, Goertz, C, Weeks, J et al. Chiropractic in North America: toward a strategic plan for professional renewal—outcomes from the 2006 Chiropractic Strategic Planning Conference. J Manipulative Physiol Ther. 2010; 33: 395–405
Lawrence, DJ, Meeker, W, Branson, R et al. Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis. J Manipulative Physiol Ther. 2008; 31: 659–674
Globe, GA, Morris, CE, Whalen, WM, Farabaugh, RJ, and Hawk, C. Chiropractic management of low back disorders: report from a consensus process. J Manipulative Physiol Ther. 2008; 31: 651–658
Baker, G, Farabaugh, RJ, Augat, TJ, and Hawk, C. Algorithms for the chiropractic management of acute and chronic spine-related pain. Top Integr Health Care. 2012; 3
Dehen, MD, Whalen, WM, Farabaugh, RJ, and Hawk, C. Consensus terminology for stages of care: acute, chronic, recurrent, and wellness. J Manipulative Physiol Ther. 2010; 33: 458–463
Farabaugh, RJ, Dehen, MD, and Hawk, C. Management of chronic spine-related conditions: consensus recommendations of a multidisciplinary panel. J Manipulative Physiol Ther. 2010; 33: 484–492
Sackett, DL, Rosenberg, WM, Gray, JA, Haynes, RB, and Richardson, WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996; 312: 71–72
Sackett, DL, Straus, SE, Richardson, WS et al. Evidence-based medicine: how to practice and teach EBM. 2nd ed. Church Livingston, Edinburgh; 2000
Slaughter, AL, Frith, K, O’Keefe, L, Alexander, S, and Stoll, R. Promoting best practices for managing acute low back pain in an occupational environment. Workplace Health Saf. 2015; 63: 408–414
Haldeman, S and Dagenais, S. What have we learned about the evidence-informed management of chronic low back pain?. Spine J. 2008; 8: 266–277
Clar, C, Tsertsvadze, A, Court, R, Hundt, GL, Clarke, A, and Sutcliffe, P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: systematic review and update of UK evidence report. Chiropr Man Ther. 2014; 22: 12
Council on Chiropractic Education. Accreditation standards, principles, processes & requirements for accreditation. (Scottsdale, AZ); 2013
Christensen, M, Kollasch, M, and Hyland, JK. Practice analysis of chiropractic. NBCE, Greeley, CO; 2010
Bronfort, G, Haas, M, Evans, R, Leiniger, B, and Triano, J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopath. 2010; 18: 3
Hawk, C, Schneider, M, Evans, MW, and Redwood, D. Consensus process to develop a best-practice document on the role of chiropractic care in health promotion, disease prevention, and wellness. J Manipulative Physiol Ther. 2012; 35: 556–567
Hawk, C, Khorsan, R, Lisi, AJ, Ferrance, RJ, and Evans, MW. Chiropractic care for nonmusculoskeletal conditions: a systematic review with implications for whole systems research. J Altern Complement Med. 2007; 13: 491–512
Hawk, C, Schneider, M, Dougherty, P, Gleberzon, BJ, and Killinger, LZ. Best practices recommendations for chiropractic care for older adults: results of a consensus process. J Manipulative Physiol Ther. 2010; 33: 464–473
Hawk, C, Schneider, M, Ferrance, RJ, Hewitt, E, Van Loon, M, and Tanis, L. Best practices recommendations for chiropractic care for infants, children, and adolescents: results of a consensus process. J Manipulative Physiol Ther. 2009; 32: 639–647
Schneider, M, Vernon, H, Ko, G, Lawson, G, and Perera, J. Chiropractic management of fibromyalgia syndrome: a systematic review of the literature. J Manipulative Physiol Ther. 2009; 32: 25–40
Vernon, H and Schneider, M. Chiropractic management of myofascial trigger points and myofascial pain syndrome: a systematic review of the literature. J Manipulative Physiol Ther. 2009; 32: 14–24
Pfefer, MT, Cooper, SR, and Uhl, NL. Chiropractic management of tendinopathy: a literature synthesis. J Manipulative Physiol Ther. 2009; 32: 41–52
Brantingham, JW, Bonnefin, D, Perle, SM et al. Manipulative therapy for lower extremity conditions: update of a literature review. J Manipulative Physiol Ther. 2012; 35: 127–166
Brantingham, JW, Cassa, TK, Bonnefin, D et al. Manipulative therapy for shoulder pain and disorders: expansion of a systematic review. J Manipulative Physiol Ther. 2011; 34: 314–346
Brantingham, JW, Cassa, TK, Bonnefin, D et al. Manipulative and multimodal therapy for upper extremity and temporomandibular disorders: a systematic review. J Manipulative Physiol Ther. 2013;36: 143–201
Brantingham, JW, Globe, G, Pollard, H, Hicks, M, Korporaal, C, and Hoskins, W. Manipulative therapy for lower extremity conditions: expansion of literature review. J Manipulative Physiol Ther. 2009; 32: 53–71
Brantingham, JW, Parkin-Smith, G, Cassa, TK et al. Full kinetic chain manual and manipulative therapy plus exercise compared with targeted manual and manipulative therapy plus exercise for symptomatic osteoarthritis of the hip: a randomized controlled trial. Arch Phys Med Rehabil. 2012; 93: 259–267
Becker, M, Neugebauer, EA, and Eikermann, M. Partial updating of clinical practice guidelines often makes more sense than full updating: a systematic review on methods and the development of an updating procedure. J Clin Epidemiol. 2014; 67: 33–45
Shekelle, P, Woolf, S, Grimshaw, JM, Schunemann, HJ, and Eccles, MP. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci. 2012; 7: 62
The AGREE Next Steps Consortium. Appraisal of guidelines for research and evaluation II. ([Ontario, Canada]); 2013
Moher, D, Liberati, A, Tetzlaff, J, Altman, DG, and Group, P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 339: b2535
Dagenais, S, Gay, RE, Tricco, AC, Freeman, MD, and Mayer, JM. NASS contemporary concepts in spine care: spinal manipulation therapy for acute low back pain. Spine J. 2010; 10: 918–940
Dagenais, S, Tricco, AC, and Haldeman, S. Synthesis of recommendations for the assessment and management of low back pain from recent clinical practice guidelines. Spine J. 2010; 10: 514–529
Furlan, AD, Yazdi, F, Tsertsvadze, A et al. Complementary and alternative therapies for back pain II.Evid Rep Technol Assess (Full Rep). 2010; : 1–764
Goertz, CM, Pohlman, KA, Vining, RD, Brantingham, JW, and Long, CR. Patient-centered outcomes of high-velocity, low-amplitude spinal manipulation for low back pain: a systematic review. J Electromyogr Kinesiol. 2012; 22: 670–691
Hidalgo, B, Detrembleur, C, Hall, T, Mahaudens, P, and Nielens, H. The efficacy of manual therapy and exercise for different stages of non-specific low back pain: an update of systematic reviews. J Man Manip Ther. 2014; 22: 59–74
Koes, BW, van Tulder, M, Lin, CW, Macedo, LG, McAuley, J, and Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010; 19: 2075–2094
McIntosh, G and Hall, H. Low back pain (acute). BMJ Clin Evid. 2011; 2011
Posadzki, P and Ernst, E. Spinal manipulations for cervicogenic headaches: a systematic review of randomized clinical trials. Headache. 2011; 51: 1132–1139
Rubinstein, SM, Terwee, CB, Assendelft, WJ, de Boer, MR, and van Tulder, MW. Spinal manipulative therapy for acute low back pain: an update of the cochrane review. Spine (Phila Pa 1976). 2013; 38: E158–E177
Rubinstein, SM, van Middelkoop, M, Assendelft, WJ, de Boer, MR, and van Tulder, MW. Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review. Spine (Phila Pa 1976). 2011; 36: E825–E846
Haas, M, Vavrek, D, Peterson, D, Polissar, N, and Neradilek, MB. Dose-response and efficacy of spinal manipulation for care of chronic low back pain: a randomized controlled trial. Spine J. 2014;14: 1106–1116
Senna, MK and Machaly, SA. Does maintained spinal manipulation therapy for chronic nonspecific low back pain result in better long-term outcome?. Spine (Phila Pa 1976). 2011; 36: 1427–1437
von Heymann, WJ, Schloemer, P, Timm, J, and Muehlbauer, B. Spinal high-velocity low amplitude manipulation in acute nonspecific low back pain: a double-blinded randomized controlled trial in comparison with diclofenac and placebo. Spine (Phila Pa 1976). 2013; 38: 540–548
Walker, BF, Hebert, JJ, Stomski, NJ, Losco, B, and French, SD. Short-term usual chiropractic care for spinal pain: a randomized controlled trial. Spine (Phila Pa 1976). 2013; 38: 2071–207
Ernst, E. Chiropractic spinal manipulation: what does the ‘best’ evidence show?. Focus Altern Complement Ther. 2012; 17: E463–E472
Menke, JM. Do manual therapies help low back pain? A comparative effectiveness meta-analysis.Spine (Phila Pa 1976). 2014; 39: E463–E472
Chou, R, Fu, R, Carrino, JA, and Deyo, RA. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet. 2009; 373: 463–472
Chou, R and Huffman, LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007; 147: 492–504
Chou, R, Qaseem, A, Snow, V et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007; 147: 478–491
Chou, WC, Tinetti, ME, King, MB, Irwin, K, and Fortinsky, RH. Perceptions of physicians on the barriers and facilitators to integrating fall risk evaluation and management into practice. J Gen Intern Med. 2006; 21: 117–122
Guzman, J, Haldeman, S, Carroll, LJ et al. Clinical practice implications of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: from concepts and findings to recommendations. Spine. 2008; 33: S199–S213
Haas, M, Bronfort, G, and Evans, RL. Chiropractic clinical research: progress and recommendations. J Manipulative Physiol Ther. 2006; 29: 695–706
Haas, M, Jacobs, GE, Raphael, R, and Petzing, K. Low back pain outcome measurement assessment in chiropractic teaching clinics: responsiveness and applicability of two functional disability questionnaires. J Manipulative Physiol Ther. 1995; 18: 79–87
Haas, M, Sharma, R, and Stano, M. Cost-effectiveness of medical and chiropractic care for acute and chronic low back pain. J Manipulative Physiol Ther. 2005; 28: 555–563
Haldeman, S, Carroll, L, Cassidy, JD, Schubert, J, and Nygren, A. The Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: executive summary. Spine (Phila Pa 1976). 2008; 33: S5–S7
in: S Haldeman, D Chapman-Smith, DJ Petersen (Eds.) Guidelines for chiropractic quality assurance and practice parameters. Aspen Publishers, Gaithersburg, MD; 1993
Haldeman, S and Dagenais, S. A supermarket approach to the evidence-informed management of chronic low back pain. Spine J. 2008; 8: 1–7
Fitch, K, Bernstein, SJ, Aquilar, MS et al. The RAND UCLA Appropriateness Method user’s manual.RAND Corp., Santa Monica, CA; 2003
American Medical Association. Guide to the evaluation of permanent impairment. 6th ed. American Medical Association, Chicago; 2008
Schneider, M, Haas, M, Glick, R, Stevans, J, and Landsittel, D. Comparison of spinal manipulation methods and usual medical care for acute and subacute low back pain: a randomized clinical trial.Spine (Phila Pa 1976). 2015; 40: 209–217
National Institute for Health and Care Excellence. Early management of persistent non-specific low back pain. NICE, UK; 2009
van Duijvenbode, I, Jellema, P, van Poppel, MN, and van Tulder, MW. Lumbar supports for prevention and treatment of low back pain. Cochrane Database Syst Rev. 2011; : CD001823
Triano, J, Budgell, B, Bagnulo, A et al. Review of methods used by chiropractors to determine the site for applying manipulation. Chiropr Man Ther. 2013; 21: 36
Carnes, D, Mars, TS, Mullinger, B, Froud, R, and Underwood, M. Adverse events and manual therapy: a systematic review. Man Ther. 2010; 15: 355–363
Dabbs, V and Lauretti, WJ. A risk assessment of cervical manipulation vs. NSAIDs for the treatment of neck pain. J Manipulative Physiol Ther. 1995; 18: 530–536
Boswell, MV, Trescot, AM, Datta, S et al. Interventional techniques: evidence-based practice guidelines in the management of chronic spinal pain. Pain Physician. 2007; 10: 7–111
Deyo, RA, Dworkin, SF, Amtmann, D et al. Report of the NIH task force on research standards for chronic low back pain. Spine (Phila Pa 1976). 2014; 39: 1128–1143
Russell, R. The rationale for primary spine care employing biopsychosocial, stratified and diagnosis-based care-pathways at a chiropractic college public clinic: a literature review. ([Online access only 11 p.])Chiropr Man Ther. 2013; 21
Revicki, D, Hays, RD, Cella, D, and Sloan, J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol. 2008; 61: 102–109
Bush, HM, Pagorek, S, Kuperstein, J, Guo, J, Ballert, KN, and Crofford, LJ. The association of chronic back pain and stress urinary incontinence: a cross-sectional study. J Womens Health Phys Ther. 2013;37: 11–18
Bi, X, Zhao, J, Zhao, L et al. Pelvic floor muscle exercise for chronic low back pain. J Int Med Res. 2013; 41: 146–152
Parkin-Smith, GF, Norman, IJ, Briggs, E, Angier, E, Wood, TG, and Brantingham, JW. A structured protocol of evidence-based conservative care compared with usual care for acute nonspecific low back pain: a randomized clinical trial. Arch Phys Med Rehabil. 2012; 93: 11–20
Peterson, CK, Bolton, J, and Humphreys, BK. Predictors of outcome in neck pain patients undergoing chiropractic care: comparison of acute and chronic patients. Chiropr Man Therap. 2012;20: 27
Peterson, CK, Bolton, J, and Humphreys, BK. Predictors of improvement in patients with acute and chronic low back pain undergoing chiropractic treatment. J Manipulative Physiol Ther. 2012; 35: 525–533
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

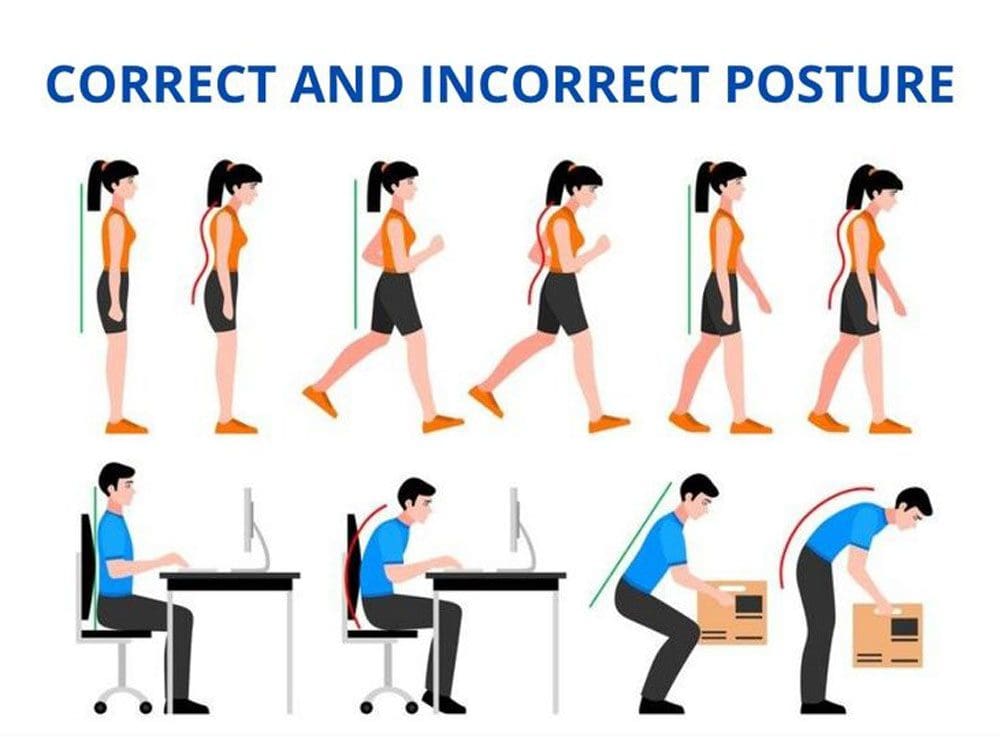 Healthy Posture Guidelines
Healthy Posture Guidelines