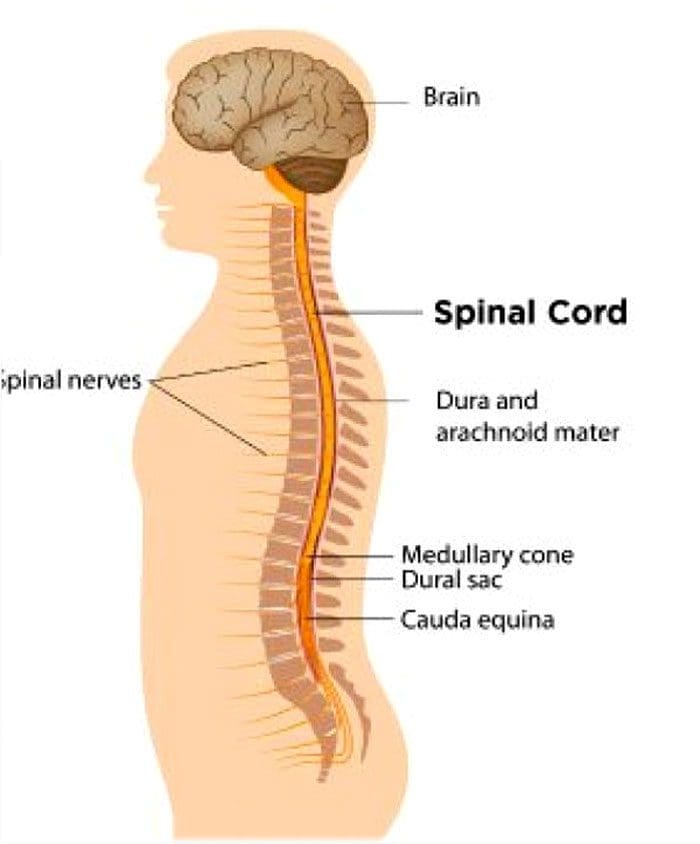
Recovery and rehabilitation after spinal fusion surgery take time. Gentle yoga poses can help expedite recovery from spinal fusion surgery and are recommended in a rehabilitation program. The spine is the body’s central support structure that allows the body to stand upright, bend, and stay balanced. However, an individual may need to have vertebrae fused to repair painful back problems. Spinal fusion is a surgical procedure that permanently connects/fuses two or more vertebrae into a single bone. The procedure is done to help:
Correct a deformity
Improve stability
Reduce pain
At the beginning of the recovery process, the doctor may recommend light physical activity like walking. As the spine continues to heal, moderate exercise is essential for optimal recovery. Doctors are recommending gentle yoga to increase mobility, flexibility and regain strength.
Gentle Yoga and Spine Surgery Recovery
Yoga has become a way to stretch the body, exercise, promote physical and mental well-being. There are different styles of yoga, ranging from gentle stretching to advanced poses. Yoga focuses on stretching, coordination, and balance. When stretching the body, the range of motion is improved. Yoga also helps improve balance and increases strength to reduce the risk of falls and injuries. Gentle yoga after spinal fusion benefits include:
Pain relief
Stress reduction
Improved mental health
Increased flexibility and strength
Improved balance
Increase in energy levels
Gentle yoga after surgery focuses on an improved range of motion/coordination of the arms and legs with the torso. This allows the spine to safely flex, not become stiff, and avoid strain, leading to fuller activity.
When To Begin Yoga After Spinal Fusion?
A reduced range of motion and loss of muscle mass is expected in the weeks and months following surgery. The healthcare/rehabilitation team will address this through exercise and physical therapy once the doctor clears the individual to begin rehabilitation training. The doctor will use some form of diagnostic imaging to determine if the vertebrae have fully fused before giving the ok for exercise. Most individuals can begin light physical activity four to six weeks after the procedure. If the fusion surgery was fused in only one place, individuals could start gentle yoga poses within two to three months. For a multi-level fusion surgery, individuals may need to wait four to six months after the procedure before they can safely begin.
Yoga Recovery Program
It’s essential to take it slow and steady when first beginning yoga after spinal fusion. As the body continues to heal, gradually add more challenging poses and stretches to the routine. This is a graduated recovery program separated into stages to help the individual build back strength and flexibility. In the first stages of recovery, gentle poses that have minimal effects on the spine are recommended. These include:
It’s crucial to listen to the body as a guide when moving through the poses, no matter what stage of recovery. The fusion needs time to heal and stabilize, so any poses that involve twisting movements and flexing should be avoided. Seek advice if there is confusion about how or whether or not to proceed. It is recommended to work with an experienced yoga teacher after spinal fusion. A knowledgeable instructor can guide with the poses, inform which poses to avoid and make modifications to get the most out of the gentle poses.
Body Composition
How Heat Affects Basal Metabolic Rate
Gender, height, and age influence Basal Metabolic Rate. These are factors individuals cannot control or change. However, individuals can increase the calories the body burns by regulating body temperature. Both the internal and external temperatures influence metabolic rate. The chemical reactions that contribute to metabolism happen more quickly if the temperature is higher, as the body works harder to restore normal temperature balance. For example, when a fever is present, the Basal Metabolic Rate will jump up to a much higher rate than usual to increase the speed of cellular metabolic reactions to combat the fever and get the body back to a healthy state. When it comes to external temperature, it’s only prolonged exposure to heat that raises the Basal Metabolic Rate.
Gillooly, James F, and Andrew P Allen. “Changes in body temperature influence the scaling of VO2max and aerobic scope in mammals.” Biology letters vol. 3,1 (2007): 99-102. doi:10.1098/rsbl.2006.0576
Individuals that go through severe low back pain caused by degeneration, herniated discs, vehicle, personal, work, and sports injuries, surgery, or spinal fusion is usually a last resort if non-invasive treatments fail to provide relief or not enough relief. Patients try to avoid spinal fusion because it can be an intense experience and requires a year-long recovery period. Unfortunately, individuals still experience discomfort and pain after surgery. Do individuals want to know what other treatment options are available, including chiropractic care?
Doctors will inform post-op patients of the risks involved with chiropractic therapy. However, chiropractic medicine can bring natural pain relief after surgery. Chiropractic treatment requires that an individual be adequately or fully healed before beginning a personalized treatment plan. At Injury Medical Chiropractic and Functional Medicine Clinic, we consult patients post-surgery about the effectiveness of rehabilitation spinal adjustments and physical therapy massage.
Wait Time After Surgery
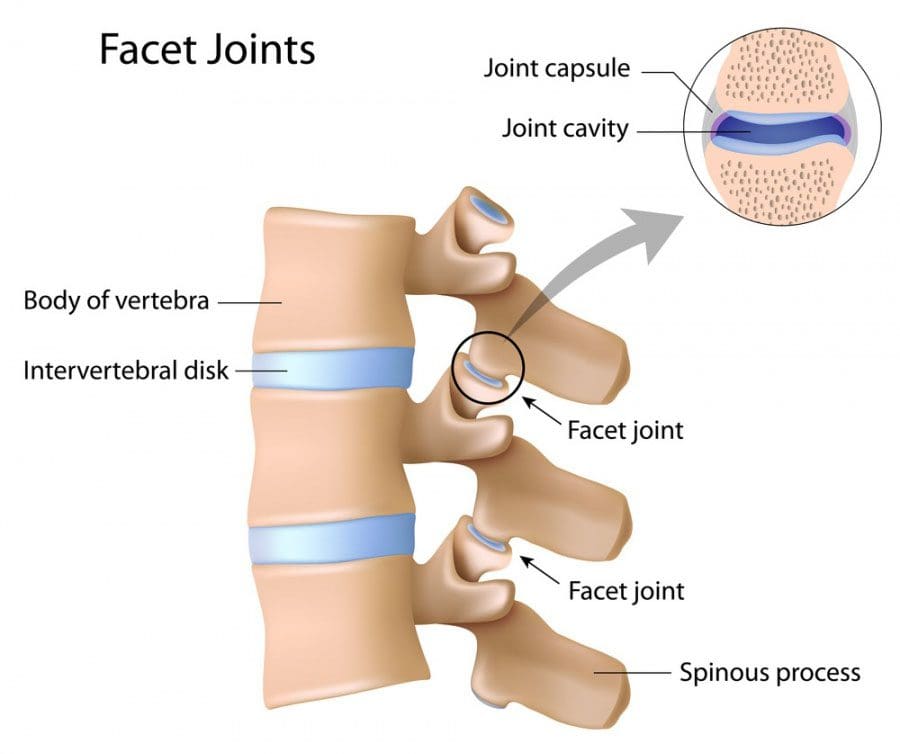
Spinal fusion surgery involves removing the discs between two or more vertebrae and fusing the bones with metal screws and plates. The objective is to correct conditions like herniated discs and degenerative diseases by immobilizing the spine in that area. It can take at least three months for the vertebrae to fuse for a fully immobilized graft. Once the graft is complete, a few months of physical therapy are recommended to loosen/stretch and strengthen the muscles around the graft. Initial recovery combined with physical therapy typically takes a full year for a complete recovery.
It is during recovery where it can be difficult and for discomfort and pain to present. The reason is patients are recommended to avoid any twisting, bending, over-reaching motions, or the graft could break. This can make an individual take on awkward poses/postures, flexing and contracting muscles incorrectly, causing strain. The result is added discomfort and/or pain.
How Chiropractic Helps
Spinal fusion is not guaranteed to alleviate an individual’s back pain completely. But many do experience discomfort or pain post-surgery. This could be for a little while or longer, depending on their condition or injuries. Fortunately, chiropractic treatment can help bring pain relief through mobilization, manipulation, and massage techniques. Manipulations’ objective is to adjust and/or realign the bones of the spine and other areas of the body. Because of the intricacy of spinal manipulations, many who have undergone back or spinal fusion surgery are hesitant to seek chiropractic treatment. Discuss possible chiropractic care with your physician to determine if the surgical graft is strong enough to withstand spinal manipulations. If the graft is adequately/fully healed and your physician believes it can endure mild adjustments, reach out to a chiropractor to discuss a customized treatment plan.
Body Composition Testing
Poor Leg Skeletal Muscle Mass
The gluteal muscles or buttock muscles are the largest muscle group in the body. Individuals can start losing bone density by their 30s. This increases the risk of injury and further bone density loss. Bone density loss is a natural process, but the process can be accelerated for individuals with under-developed skeletal muscle mass. The health of muscles and bones are closely linked. Researchers found that individuals with less muscle mass than average for their height tended to have narrower and thinner bones. This resulted in limited lower bending strength.
Decreased muscle mass was shown to be linked to balance problems and increased risk of falls. There is a higher prevalence of sarcopenia or muscle wasting for patients with hip fractures and a reduction of leg muscle mass. The combination of:
Low muscle mass
Low bone density
Hip fractures
It can have lifelong consequences
References
Fernandez, Matthew et al. “Surgery or physical activity in the management of sciatica: a systematic review and meta-analysis.” The European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 25,11 (2016): 3495-3512. doi:10.1007/s00586-015-4148-y
Keller, Glenda. “The effects of massage therapy after decompression and fusion surgery of the lumbar spine: a case study.” International journal of therapeutic massage & bodywork vol. 5,4 (2012): 3-8. doi:10.3822/ijtmb.v5i4.189
O’Shaughnessy, Julie et al. “Chiropractic management of patients post-disc arthroplasty: eight case reports.” Chiropractic & osteopathy vol. 18 7. 21 Apr. 2010, doi:10.1186/1746-1340-18-7
Perrucci, Rachel M, and Christopher M Coulis. “Chiropractic management of post-spinal cord stimulator spine pain: a case report.” Chiropractic & manual therapies vol. 25 5. 6 Feb. 2017, doi:10.1186/s12998-017-0136-0
Szulc, Pawel et al. “Low skeletal muscle mass is associated with poor structural parameters of bone and impaired balance in elderly men–the MINOS study.” Journal of bone and mineral research: The American Society for Bone and Mineral Research vol. 20,5 (2005): 721-9. doi:10.1359/JBMR.041230
Many doctors/surgeons rely on the widely adopted lumbar spinal fusion. However, experts have asserted that lumbar total disc replacement or TDR should be made available and increased for treating degenerative disc disease and other spinal conditions. Individuals interested in total disc replacement, the ability to have it done, and if insurance will pay? What to know about TDR and fusion before deciding and moving forward.
Total Disc Replacement
Spinal fusion has been the traditional approach for relieving lower back pain. In this procedure, a bone graft is inserted between two or more vertebrae. This eliminates movement that causes pain or could be dangerous to the individual. Total disc replacement demands more on a technical level than spinal fusion. However, the worn-out, injured, or damaged disc is fully replaced, even a completely degenerated disc, with a metal and/or plastic one. Benefits from lumbar TDR surgery include:
Shown to be a safe procedure with minimal complications
Significant improvement in health and quality of life
High rates of successful outcomes
Mobility is preserved
Who Needs Disc Replacement?
Low back problems affect more than a third of the population. This can come from:
Personal
Work
Sports
Automobile injuries
Aging
All are risk factors
Fusion or Total disc replacement
Fusion reduces and eliminates motion around the affected area which also changes with the spine’s mechanics. It can also place increased stress on the surrounding segments. However, the lack of motion is to eliminate the pain. Total disc replacement does increase mobility, but it can’t fully relieve the pain. It can relieve pain generated from the disc but not from other causes. TDR has been shown to:
Provides motion preservation
Reduces staying at the hospital
Provides long-term durability
Lower reoperation rates compared to fusion
Total disc replacement issues:
The procedure is more time-consuming
A lot of time making decisions
A lot of time preparing
An example could be the patient has a narrow disc space. Looking at the X-rays of the discs above and below, the surgeon has to make sure they choose the right size. Next, the narrow space needs to be mobilized back to a normal height that cannot be too high or too short. Finally, the surgeon has to make sure that the disc is anchored and fits properly.
Why Surgeons Still Choose Fusion?
Despite the benefits, there are reasons why surgeons still choose fusion.
There are strict rules as to when TDR can be used. This means insurers are prone only to approve fusion procedures.
The surgical technique is challenging. TDR surgery is a highly demanding procedure. As a result, many doctors specializing in fusion for 20 years or more can be reluctant to perform the procedure.
Complications and revision surgeries. Reoperations are sometimes necessary, but this happens in both fusion and TDR.
Individual Needs
Fortunately, most individuals with lower back problems never need total disc replacement. And those that do have severe pain/conditions are recommended to try non-invasive/surgical treatment. This ranges from:
Chiropractic
Physical therapy
Massage
Imaging and lab tests will be required. However, if an operation is necessary, ask questions about both procedures. For example, if a surgeon insists that fusion is the only option, ask why total disc replacement is not an option?
Body Composition Testing
Protein and Weight Loss
Protein is one of three basic macronutrients found in food. Proteins are made up of smaller units called amino acids. There are 22 amino acids, with 9 of these being essential. This means the body needs them, as the body cannot produce them. These essential amino acids can be obtained by eating protein-rich foods like:
Eggs
Meat
Fish
Vegetarian/vegan options include:
Nuts
Seeds
Beans
Tofu
Generally, all the essential amino acids cannot be obtained from just one food. Therefore it is recommended to eat a variety of animal and plant-based proteins. Protein is in almost every structure and function of the body.
Antibodies
These proteins fight off any infections, bacteria, etc.
Repair, maintenance, and structural
Proteins are the building blocks of the body’s muscles, bones, skin, and hair.
Hormones
Chemical messenger proteins are how cells and organs communicate. For example, Growth Hormone affects muscle gain and fat loss.
Enzymes
Not all proteins are enzymes; however, all enzymes are proteins. These proteins are catalysts or starters for chemical reactions in the body.
Transportation and storage
Some proteins carry molecules where they are needed. For example, hemoglobin or the red blood cells carry oxygen to cells, then transport carbon dioxide away.
Not getting enough protein in one’s diet can have serious consequences on the body’s health. Without enough protein, the muscles can begin to atrophy or waste away, taking Lean Body Mass, strength, and energy away as well.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. In addition, we provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Salzmann, Stephan N et al. “Lumbar disc replacement surgery-successes and obstacles to widespread adoption.” Current reviews in musculoskeletal medicine vol. 10,2 (2017): 153-159. doi:10.1007/s12178-017-9397-4
“Comparison of Lumbar Total Disc Replacement With Surgical Spinal Fusion for the Treatment of Single-Level Degenerative Disc Disease: A Meta-Analysis of 5-Year Outcomes From Randomized Controlled Trials”, Zigler J, et al., Global Spine Journal, June 2018, PMC602295 www.ncbi.nlm.nih.gov/pmc/articles/PMC6022955/
A bone graft is defined as using bone-in spine fusion surgery. Spinal fusion’s purpose is to link or weld bones together, in this case, the spinal bones. There are a variety of spinal conditions cause instability and pain:
Degenerative disc disease
Scoliosis
Trauma from an auto accident, sports injury, slip, and fall accident
Spine surgeons use a bone graft to:
Stop motion between two or more vertebrae
Stabilize a spinal deformity
Repair fractures of the spine
�
�
Spinal Fusion Stimulates New Bone Growth
A bone graft does not heal or fuse the spine instantly. Rather a bone graft sets up a foundational frame for the individual’s body to generate and grow new bone. A bone graft stimulates new bone production. It is when this new bone begins to grow and solidify, that fusion takes place.
With these types of surgeries, instrumentation like screws, and rods are typically used for the beginning stabilization. But it is the actual healing of the bone that welds the vertebrae together creating long-term stability.
A bone graft can be used for structural purposes for supporting the spine, usually this is done in place of a disc or bone that was removed. Or it can be an onlay, this means that a mass of bone fragments will grow together to stabilize the spine bridging the joint.
There are two generalized bone graft types:
Real bone
Substituted bone graft
Real bone can come from the patient, which is called an auto-graft or from a donor’s bone, called an allograft.
�
The Individual’s Bone or Auto-graft
An auto-graft is bone taken or harvested from the individual’s body and transplanted to a specific area, in this case, the spine. An auto-graft is considered the gold standard because it is the individual’s own bone, which contains:
These all help to stimulate the healing of the fusion. There are advantages for an auto-graft, which include a higher probability for fusion success and a lower risk for disease transmission. The only real setback for individuals of an auto-graft is the post-operative pain that usually comes with the procedure when harvesting an individuals’ bone. Bone can be harvested from one of the individual’s:
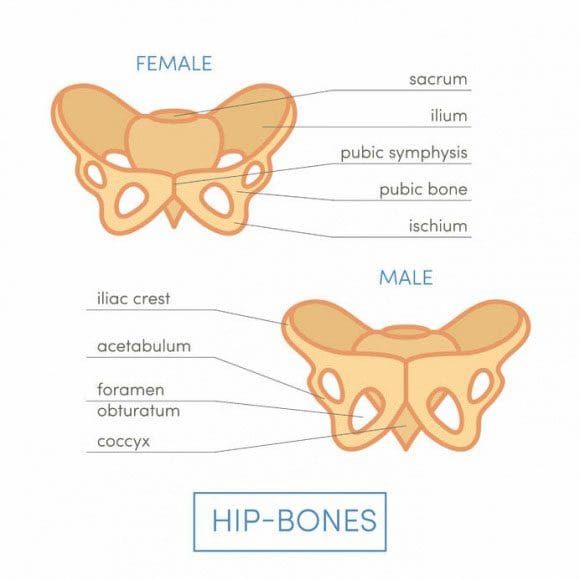
Iliac crests
Pelvic bones
Ribs
Spine
� Bone graft harvesting creates a new set of risks. These include:
Because of these risks and the possibility that the bone could be poor quality, a surgeon could decide to use another type of bone graft. When this happens a surgeon could go with what is known as a local auto-graft. This is bone harvested from the decompression itself.
These are the parts that are removed to decompress the nerves. They usually consist of bone spurs, lamina, and portions of the spinous process. These same bone pieces can be reused to assist with the fusion of the decompressed areas.
�
Donor Bone or Allograft
An allograft is a bone harvested from another person, usually from a tissue bank. Tissue banks harvest bone and other tissues from cadavers for medical purposes. An allograft is prepared by freezing or freeze-drying the bone or tissues. This helps limit the risk of graft rejection. Bone from an allograft does not have living bone cells and is not as effective at fusion stimulation when compared to an autograft. However, it still does work. Tissue banks:
Screen all their donors
Supervise bone recovery
Test donations
Sterilize donations
Store for use
Look for tissue banks that are accredited by the American Association of Tissue Banks. US Food and Drug Administration has strict regulations when it comes to human cell and tissue processing. These include rules about the eligibility of donors. These guidelines/protocols help reduce the risk of tissue contamination and the spread of disease.
�
Bone Graft Substitute
These substitutes are man-made or are made from a manipulated version of a natural product. These alternatives are safe and can provide a solid foundation for the individual’s body to grow bone. Substitutes have similar properties of human bone, which include a porous structure and proteins that stimulate healing.
�
Demineralized Bone Matrix – DBM
A demineralized bone matrix is an allograft that has gone through a process where the mineral content has been removed. This demineralization helps reveal bone-forming proteins like collagen, and growth factors hidden within the bone that can stimulate healing.
This procedure is often considered a bone graft extender. It is not considered a replacement. This is because its ability to fuse the human spine on its own has not been proven. DBM can be combined with the regular bone for more volume and is available in these forms:
Chip
Granule
Gel
Powder
Putty
�
Ceramic-based Extenders
Ceramic-based extenders are mixed in combination with other sources of bone. This is because they consist of calcium matrix for fusion, but there are no cells or proteins to stimulate the healing process. These include:
Ceramic-based extenders do not present a risk for disease transfer but can cause inflammation. They are available in porous and mesh forms.
�
Morphogenetic Protein – BMP
Different types of bone morphogenetic proteins or BMP’s are used to stimulate new bone growth. These proteins are found in human bone, however, they are trace amounts. They are then produced in larger amounts through genetic engineering.
This all depends on the type of spine surgery an individual undergoes. Bone morphogenetic protein could be considered an option in promoting new bone growth along with healing fusion.
Anterior cervical discectomy and fusion (ACDF)�is a procedure that treats chronic neck conditions and is the most common spinal surgery performed in the U.S.�30 percent of Americans a year experience neck pain, chronic neck pain and radiculopathy or pain that spreads out and radiates to other parts of the body, in this case down the arms.
It�s a procedure that can work wonders, but as many as two-thirds of patients continue to manage neck pain and dysfunction after ACDF. One of the best ways of managing neck pain and dysfunction is to exercise. Research shows that a prescribed exercise program right after surgery can help lessen the pain and create less dependence on medications. A 2020 study published in SPINE suggests that patients that began therapeutic exercises right away had better results than individuals that started an exercise program after the six-week checkup/examination.
What Anterior Cervical Discectomy Fusion Treats
The procedure is performed on individuals with degenerative disc disease or a bulging or herniated disc. These conditions can cause the spinal disc to place pressure on the spinal cord and nerve roots that branch out, creating:
Numbness
Tingling
Pain
Weakness in one or both arms
Most individuals that are recommended to undergo the surgery experience symptoms that don�t respond to non-surgical therapies or medication/s. A significant symptom is hand/arm weakness and arm pain that�s worse than the neck pain.
ACDF Surgery
The ACDF procedure is broken into two parts: a discectomyand a fusion. Anterior means in front and in this case it’s the front of the neck that the surgeon accesses the damaged discs.�In a discectomy, the surgeon removes a portion/s or all of an intervertebral disc/s to release the pressure on the nerves. The fusion part fuses the two vertebrae together. This eliminates the painful movements. A bone graft is inserted between the vertebrae at the spot where the disc was removed. The bone graft serves as a structural scaffold that the body uses to build new tissue and cause the vertebrae to grow together.
The graft can come from three sources:
Your own bone called an autograft, this is usually a piece of bone from the pelvis just above where the front jean pocket would be.
Bone donation called an allograft that comes from a cadaver from a bone donor bank.
Substitute material/s like man-made plastic, ceramic, or bioresorbable compounds.
Home Exercise Program
There are those that are of the opinion to hold off on physical therapy or exercise until about six weeks post-ACDF when recovery is established. However, the study suggests it is more effective to begin a home exercise program (HEP) as soon as possible. At this time telemedicine is the replacement for in-person physical therapy sessions but works just as well. The study examined 28 individuals’ outcomes over 12-months post-operation.
The participants were divided into two groups:� Standard care and Early HEP. Both groups went through the standard postoperative care, along with medication, a cervical collar or neck brace, and restrictions of certain activities. The standard care group received physical therapy referral six weeks after surgery while the early HEP group was given a home exercise program to perform during the postoperative six-weeks.
This included walking and sleeping instructions and a range of motion/strengthening exercises. A cognitive-behavioral strategy was also given to help relax. The participants would phone-conference with a physical therapist on a weekly basis. Exercises increased in difficulty every two weeks, based on the therapists’ judgment. When compared to the standard care group, the early HEP group reported a reduction in short-term neck pain and were less likely to be using pain meds/opioids twelve months after their surgery.
Recovery Tips
Recovery time after ACDF surgery typically lasts about four to six weeks. If the bone graft was from the pelvis, there could be pain, soreness, and stiffness. To minimize discomfort, try not to sit or lie down for long periods. And remember to change position or take a quick short walk down the hall, to the kitchen, etc. every 20-30 minutes. If you are referred to physical therapy combine it with the home exercise program. The therapist will teach you exercises and proper form. Exercising ten minutes every day is far more effective than doing 45 minutes once a week.
Resuming normal activities gradually is crucial. No pain, no gain does not apply when recovering from ACDF surgery. Recovery exercises can feel great. However, pain and fatigue can sneak up the next day or the following week. Gradually easing back into daily activities can help avoid major setbacks. Work, shopping, house chores, childcare, and lawn care all fall into the activity category.
A recurrence of neck pain after recovery is normal. However,�discomfort can be minimized by taking a few precautions.
Use proper form when lifting
Keep objects close to the body
Keep the back flat as you lift
Maintain neutral neck position
Be aware of your posture when sitting, standing, walking, and sleeping
Gradually increase the exercise program
Don’t overdo it
Address underlying fear/anxiety
Fear of generating pain can cause tension and exacerbate or even create new pain symptoms
Stop smoking, as it has shown to impede the fusion and heighten the risk for complications
ACDF surgery can improve quality of life. Your surgeon is responsible for performing the procedure, it�s up to the individual to follow through with an exercise program and proper ergonomics for optimal results.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine