Nerves control muscle fibers. Muscle twitching is an involuntary contraction of the muscle fibers. When individuals play sports/work out vigorously or for a long time, they may experience muscle twitching and can often see and/or feel the twitches happening. The most worked-out muscles are likely to twitch, which includes the biceps, thighs, and calves, but twitches can occur in any muscle. Chiropractic care, massage therapy, and functional medicine can help relax the muscles, improve circulation, restore function, and train individuals to prevent future episodes.
Muscle Twitching
A muscle twitch often occurs after intense physical activity or a hard workout because the muscle or muscles have been overworked, and there is hyper-excitability of the nerve/s that makes the muscle/s continue to contract.
A muscle twitch that can be seen is called fasciculation.
A muscle twitch that cannot be seen is called fibrillation.
If there is pain or the twitching is prolonged, it is a muscle spasm.
Causes
The most common causes include the following:
Intense exercise and rigorous physical activity build up lactic acid in the muscles.
Dehydration is a very common factor for shaky muscles.
Vitamin D and calcium deficiencies could cause muscle spasms in the hand, calves, and eyelids.
Using caffeinated products to increase physical performance.
Not enough or a lack of healthy sleep.
Anxiety or stress.
Certain medications like estrogen and corticosteroids.
Nicotine and tobacco use.
Physical Activity/Exercise
Intense exercise and physical activity can cause muscle fatigue.
Muscle fatigue triggers twitching and cramping in overworked muscle fibers.
Electrolytes play a role in muscle contraction.
Electrolyte loss and imbalances within muscle fibers through sweating can lead to twitching.
Dehydration
Muscle mass comprises 75% water.
Water carries nutrients and minerals to muscles to support function.
Not being properly hydrated can cause twitching and cramping.
Vitamin D Deficiency
Nerves need vitamin D to relay messages to and from the brain to the body’s muscles.
A vitamin D deficiency can cause muscle weakness and twitching.
Lack of sleep can affect neurotransmitter function.
A common site of fasciculation tiredness occurs in the eyelids.
Anxiety and Stress
Experiencing psychological stress or high anxiety levels can cause excess muscle tension.
This can lead to muscle twitching.
Muscle fasciculation caused by stress can occur anywhere in the body.
Certain Medications
Certain medications can lead to involuntary muscle twitching.
The reaction can be a side effect due to interactions with other medications.
Individuals should discuss side effects and medication interactions with their doctor when taking a new medication.
Chiropractic Care
Chiropractors are experts on the musculoskeletal system and have many techniques to treat muscle fasciculation and spasms. It often depends on the cause/s, and specific treatment varies on a case-by-case basis. Common chiropractic treatments include:
Massage therapy
Heat and ice therapy
Manual manipulation
Joint adjustments
Ultrasound
Stretches to keep the muscles flexible
Exercises to strengthen the muscles
Nutritional recommendations
Fasciculation
References
Bergeron, Michael F.. Muscle Cramps during Exercise-Is It Fatigue or Electrolyte Deficit?. Current Sports Medicine Reports July 2008 – Volume 7 – Issue 4 – p S50-S55 doi: 10.1249/JSR.0b013e31817f476a
Gragossian A, Bashir K, Friede R. Hypomagnesemia. [Updated 2022 May 15]. In: StatPearls [Internet]. Treasure Island (F.L.): StatPearls Publishing; 2022 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK500003/
Küçükali, Cem Ismail, et al. “Peripheral nerve hyperexcitability syndromes.” Reviews in the neurosciences vol. 26,2 (2015): 239-51. doi:10.1515/revneuro-2014-0066
Maughan, Ronald J, and Susan M Shirreffs. “Muscle Cramping During Exercise: Causes, Solutions, and Questions Remaining.” Sports medicine (Auckland, N.Z.) vol. 49, Suppl 2 (2019): 115-124. doi:10.1007/s40279-019-01162-1
Miller, Kevin C et al. “Exercise-associated muscle cramps: causes, treatment, and prevention.” Sports health vol. 2,4 (2010): 279-83. doi:10.1177/1941738109357299
Riebl, Shaun K, and Brenda M Davy. “The Hydration Equation: Update on Water Balance and Cognitive Performance.” ACSM’s health & fitness journal vol. 17,6 (2013): 21-28. doi:10.1249/FIT.0b013e3182a9570f
Abstract Objective: The purpose of this case report is to describe a patient with chronic, multisite muscle fasciculations who presented to a chiropractic teaching clinic and was treated with dietary modifications.
Clinical features: A 28-year-old man had muscle fasciculations of 2 years. The fasciculations began in his eye and progressed to the lips and lower extremities. In addition, he had gastrointestinal distress and fatigue. The patient was previously diagnosed as having wheat allergy at the age of 24 but was not compliant with a gluten-free diet at that time. Food sensitivity testing revealed immunoglobulin G�based sensitivity to multiple foods, including many different grains and dairy products. The working diagnosis was gluten neuropathy.
Intervention and outcome: Within 6 months of complying with dietary restrictions based on the sensitivity testing, the patient�s muscle fasciculations completely resolved. The other complaints of brain fog, fatigue, and gastrointestinal distress also improved.
Conclusions: This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary changes. There is strong suspicion that this case represents one of gluten neuropathy, although testing for celiac disease specifically was not performed.
Introduction:�Muscle Fasciculations
There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1
The reported prevalence of WA is variable. Prevalence ranges from 0.4% to 9% of the population.2,3 The prevalence of GS is somewhat difficult to determine, as it does not have a standard definition and is a diagnosis of exclusion. Gluten sensitivity prevalence of 0.55% is based on National Health and Nutrition Examination Survey data from 2009 to 2010.4 In a 2011 study, a GS prevalence of 10% was reported in the US population.5 In contrast to the above 2 examples, CD is well defined. A 2012 study examining serum samples from 7798 patients in the National Health and Nutrition Examination Survey database from 2009 to 2010 found an overall prevalence of 0.71% in the United States.6
Neurologic manifestations associated with negative reactions to wheat proteins have been well documented. As early as 1908, �peripheral neuritis� was thought to be associated with CD.7 A review of all published studies on this topic from 1964 to 2000 indicated that the most common neurologic manifestations associated with GS were ataxia (35%), peripheral neuropathy (35%), and myopathy (16%). 8 Headaches, paresthesia, hyporeflexia, weakness, and vibratory sense reduction were reported to be more prevalent in CD patients vs controls.9 These same symptoms were more prevalent in CD patients who did not strictly follow a GFD vs those who were compliant with GFD.
At present, there are no case reports describing the chiropractic management of patient with gluten neuropathy. Therefore, the purpose of this case study is to describe a patient presentation of suspected gluten neuropathy and a treatment protocol using dietary modifications.
Case Report
A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.
The patient originally attributed the muscle twitching to caffeine intake (20 oz of coffee a day) and stress from school. The patient denies the use of illicit drugs, tobacco, or any prescription medication but does drink alcohol (mainly beer) in moderation. The patient ate a diet high in meats, fruits, vegetables, and pasta. Eight months after the initial fasciculations began, the patient began to experience gastrointestinal (GI) distress. Symptoms included constipation and bloating after meals. He also began to experience what he describes as �brain fog,� a lack of concentration, and a general feeling of fatigue. The patient noticed that when the muscle fasciculations were at their worst, his GI symptoms correspondingly worsened. At this point, the patient put himself on a strict GFD; and within 2 months, the symptoms began to alleviate but never completely ceased. The GI symptoms improved, but he still experienced bloating. The patient�s diet consisted mostly of meats, fruit, vegetables, gluten-free grains, eggs, and dairy.
At the age of 24, the patient was diagnosed with WA after seeing his physician for allergies. Serum testing revealed elevated IgE antibodies against wheat, and the patient was advised to adhere to a strict GFD. The patient admits to not following a GFD until his fasciculations peaked in December 2011. In July of 2012, blood work was evaluated for levels of creatine kinase, creatine kinase�MB, and lactate dehydrogenase to investigate possible muscle breakdown. All values were within normal limits. In September of 2012, the patient under- went food allergy testing once again (US Biotek, Seattle, WA). Severely elevated IgG antibody levels were found against cow�s milk, whey, chicken egg white, duck egg white, chicken egg yolk, duck egg yolk, barley, wheat gliadin, wheat gluten, rye, spelt, and whole wheat (Table 1). Given the results of the food allergy panel, the patient was recommended to remove this list of foods from his diet. Within 6 months of complying with the dietary changes, the patient�s muscle fasciculations completely resolved. The patient also experienced much less GI distress, fatigue, and lack of concentration.
Discussion
The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field.
This case illustrates an unusual presentation of a widespread sensorimotor neuropathy that seemed to respond to dietary changes. Although this presentation is consistent with gluten neuropathy, a diagnosis of CD was not investigated. Given the patient had both GI and neurologic symptoms, the likelihood of gluten neuropathy is very high.
There are 3 forms of wheat protein reactivity. Because there was confirmation of WA and GS, it was decided that testing for CD was unnecessary. The treatment for all 3 forms is identical: GFD.
The pathophysiology of gluten neuropathy is a topic that needs further investigation. Most authors agree it involves an immunologic mechanism, possibly a direct or indirect neurotoxic effect of antigliadin anti- bodies. 9,10 Briani et al 11 found antibodies against ganglionic and/or muscle acetylcholine receptors in 6 of 70 CD patients. Alaedini et al12 found anti-ganglioside antibody positivity in 6 of 27 CD patients and proposed that the presence of these antibodies may be linked to gluten neuropathy.
It should also be noted that both dairy and eggs showed high responses on the food sensitivity panel. After reviewing the literature, no studies could be located linking either food with neuromuscular symp- toms consistent with the ones presented here. There- fore, it is unlikely that a food other than gluten was responsible for the muscle fasciculations described in this case. The other symptoms described (fatigue, brain fog, GI distress) certainly may be associated with any number of food allergies/sensitivities.
Limitations
One limitation in this case is the failure to confirm CD. All symptoms and responses to dietary change point to this as a likely possibility, but we cannot confirm this diagnosis. It is also possible that the�symptomatic response was not due directly to dietary change but some other unknown variable. Sensitivity to foods other than gluten was documented, including reactions to dairy and eggs. These food sensitivities may have contributed to some of the symptoms present in this case. As is the nature of case reports, these results cannot necessarily be generalized to other patients with similar symptoms.
Conclusion:�Muscle Fasciculations
This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of gluten neuropathy, although testing for CD specifically was not performed.
Brian Anderson DC, CCN, MPHa,?, Adam Pitsinger DCb
Attending Clinician, National University of Health Sciences, Lombard, IL Chiropractor, Private Practice, Polaris, OH
Acknowledgment
This case report is submitted as partial fulfillment of the requirements for the degree of Master of Science in Advanced Clinical Practice in the Lincoln College of Post-professional, Graduate, and Continuing Education at the National University of Health Sciences.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.
References:
1. Sapone A, Bai J, Ciacci C, et al. Spectrum of gluten-related
disorders: consensus on new nomenclature and classification.
BMC Med 2012;10:13.
2. Matricardi PM, Bockelbrink A, Beyer K, et al. Primary versus
secondary immunoglobulin E sensitization to soy and wheat in
the Multi-Centre Allergy Study cohort. Clin Exp Allergy
2008;38:493�500.
3. Vierk KA, Koehler KM, Fein SB, Street DA. Prevalence of
self-reported food allergy in American adults and use of food
labels. J Allergy Clin Immunol 2007;119:1504�10.
4. DiGiacomo DV. Prevalence and characteristics of non-celiac
gluten sensitivity in the United States: results from the
continuous National Health and Nutrition Examination Survey
2009-2010. Presented at: the 2012 American College of
Gastroenterology Annual Scientific Meeting; Oct. 19-24, Las
Vegas.; 2012.
5. Sapone A, Lammers KM, Casolaro V. Divergence of gut
permeability and mucosal immune gene expression in two
gluten-associated conditions: celiac disease and gluten sensitivity.
BMC Med 2011;9:23.
6. Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA,
Everhart JE. The prevalence of celiac disease in the United
States. Am J Gastroenterol 2012 Oct;107(10):1538�44.
7. Hadjivassiliou M, Grunewald RA, Davies-Jones GAB. Gluten
sensitivity as a neurological illness. J Neurol Neurosurg
Psychiatr 2002;72:560�3.
8. Hadjivassiliou M, Chattopadhyay A, Grunewald R, et al.
Myopathy associated with gluten sensitivity. Muscle Nerve
2007;35:443�50.
9. Cicarelli G, Della Rocca G, Amboni C, et al. Clinical and
neurological abnormalities in adult celiac disease. Neurol Sci
2003;24:311�7.
10. Hadjivassiliou M, Grunewald RA, Kandler RH. Neuropathy
associated with gluten sensitivity. J Neurol Neurosurg
Psychiatry 2006;77:1262�6.
11. Briani C, Doria A, Ruggero S, et al. Antibodies to muscle and
ganglionic acetylcholine receptors in celiac disease. Autoimmunity
2008;41(1):100�4.
12. Alaedini A, Green PH, Sander HW, et al. Ganglioside reactive
antibodies in the neuropathy associated with celiac disease.
J Neuroimmunol 2002;127(1�2):145�8.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1
There are 3 known types of negative reactions to wheat proteins, collectively known as wheat protein reactivity: wheat allergy (WA), gluten sensitivity (GS),�and celiac disease (CD). Of the 3, only CD is known to involve autoimmune reactivity, generation of antibodies, and intestinal mucosal damage. Wheat allergy involves the release of histamine by way of immunoglobulin (Ig) E cross-linking with gluten peptides and presents within hours after ingestion of wheat proteins. Gluten sensitivity is considered to be a diagnosis of exclusion; sufferers improve symptomatically with a gluten-free diet (GFD) but do not express antibodies or IgE reactivity.1 A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.
A 28-year-old man presented to a chiropractic teaching clinic with complaints of constant muscle fasciculations of 2 years� duration. The muscle fasciculations originally started in the left eye and remained there for about 6 months. The patient then noticed that the fasciculations began to move to other areas of his body. They first moved into the right eye, followed by the lips,�and then to the calves, quadriceps, and gluteus muscles. The twitching would sometimes occur in a single muscle or may involve all of the above muscles simultaneously. Along with the twitches, he reports a constant �buzzing� or �crawling� feeling in his legs. There was no point during the day or night when the twitches ceased.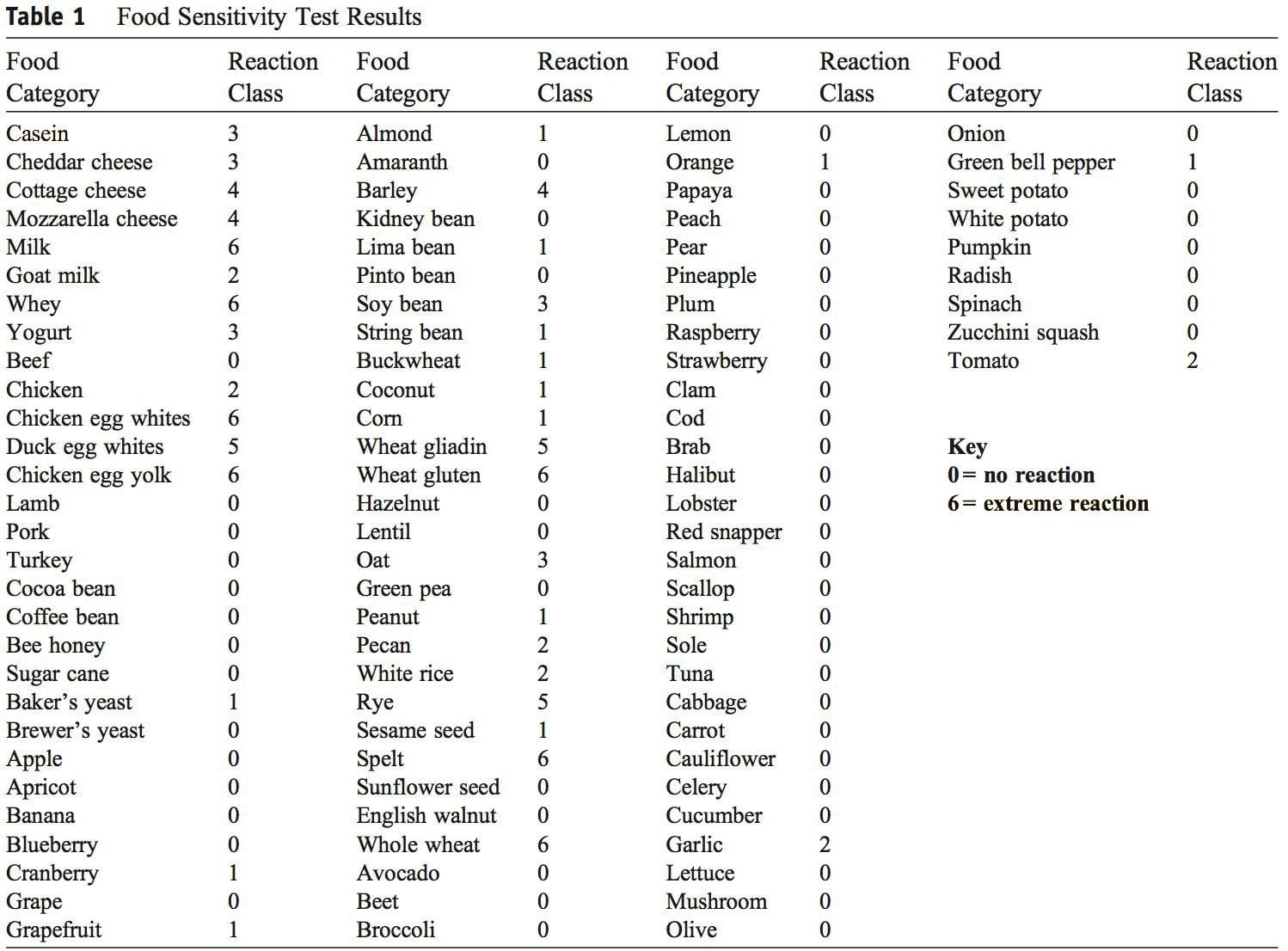 Discussion
Discussion The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field.
The authors could not find any published case studies related to a presentation such as the one�described here. We believe this is a unique presentation of wheat protein reactivity and thereby represents a contribution to the body of knowledge in this field. This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of
This report describes improvement in chronic, widespread muscle fasciculations and various other systemic symptoms with dietary change. There is strong suspicion that this case represents one of




