Back Clinic Personal Injury Chiropractic Team. Injuries from an accident can not only cause physical harm to you or a loved one, being involved in a personal injury case can often be a complicated and stressful situation to handle. These types of circumstances are unfortunately fairly common and when the individual is faced with pain and discomfort as a result of trauma from an accident or an underlying condition that has been aggravated by the injury, finding the right treatment for their specific issue can be another challenge on its own.
Dr. Alex Jimenez’s compilation of personal injury articles highlights a variety of personal injury cases, including automobile accidents resulting in whiplash, while also summarizing various effective treatments, such as chiropractic care. For more information, please feel free to contact us at (915) 850-0900 or text to call Dr. Jimenez personally at (915) 540-8444.
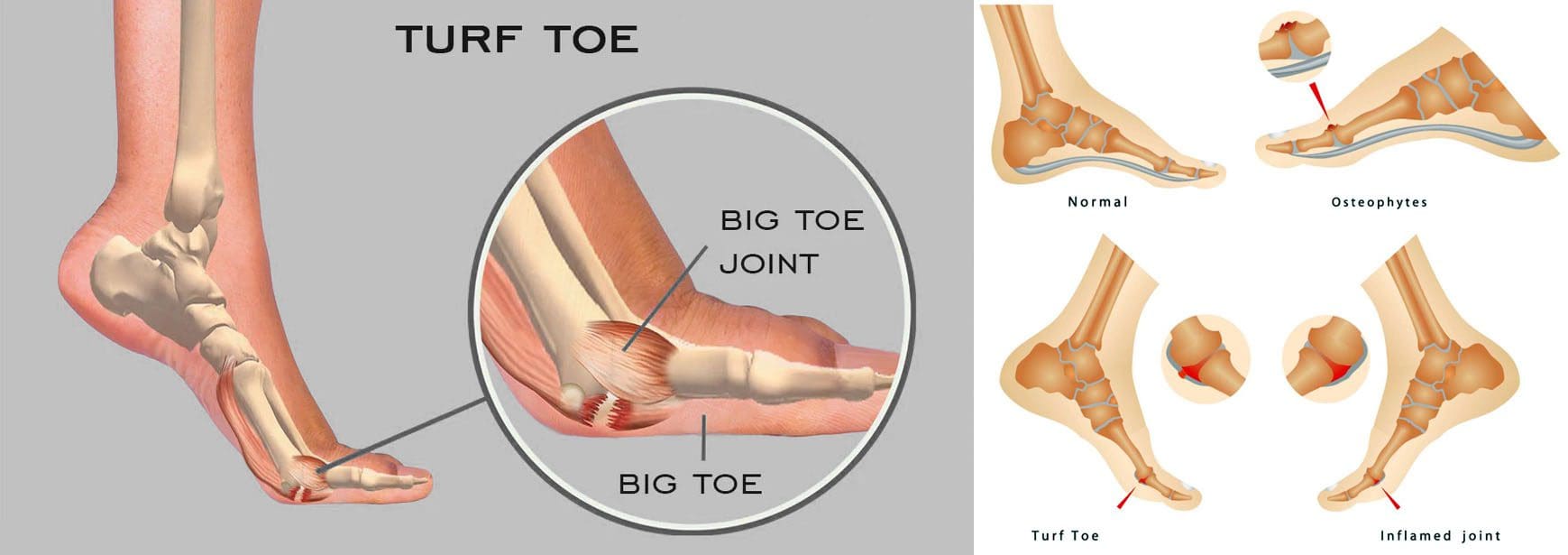
For individuals experiencing a turf toe injury, can knowing the symptoms help athletes and non-athletes with treatment, recovery time, and returning to activities?
Turf Toe Injury
A turf toe injury affects the soft tissue ligaments and tendons at the base of the big toe under the foot. This condition usually occurs when the toe is hyperextended/forced upward, such as when the ball of the foot is on the ground and the heel is lifted. (American Academy of Orthopaedic Surgeons. 2021) The injury is common among athletes who play sports on artificial turf, which is how the injury got its name. However, it can also affect non-athletes, like individuals working on their feet all day.
Recovery time after turf toe injury depends on the severity and the type of activities the individual plans to return to.
Returning to high-level sports activities after a severe injury can take six months.
These injuries vary in severity but usually improve with conservative treatment. In severe cases, surgery could be required.
Pain is the primary issue that stops physical activities after a grade 1 injury, while grades 2 and 3 can take weeks to months to heal completely.
Meaning
A turf toe injury refers to a metatarsophalangeal joint strain. This joint comprises ligaments that connect the bone on the sole of the foot, below the big toe/proximal phalanx, to the bones that connect the toes to the larger bones in the feet/metatarsals. The injury is usually caused by hyperextension that often results from a pushing-off motion, like running or jumping.
If experiencing turf toe symptoms, see a healthcare provider for a proper diagnosis so they can develop a personalized treatment plan. They will perform a physical exam to assess pain, swelling, and range of motion. (American Academy of Orthopaedic Surgeons. 2021) If the healthcare provider suspects tissue damage, they may recommend imaging with X-rays and (MRI) to grade the injury and determine the proper course of action.
Grades 2 and 3 come with partial or complete tissue tearing, severe pain, and swelling. Treatments for more severe turf toe can include: (Ali-Asgar Najefi et al., 2018)
Limited weight bearing
Using assistive devices like crutches, a walking boot, or a cast.
Physical therapy also includes proprioception and agility training exercises, orthotics, and wearing recommended shoes for specific physical activities. (Lisa Chinn, Jay Hertel. 2010)
A physical therapist can also help ensure that the individual does not return to physical activities before the injury is fully healed and prevent the risk of re-injury.
Grade 1 – Subjective as it varies depending on the individual’s pain tolerance.
Grade 2 – Four to six weeks of immobilization.
Grade 3 – Eight weeks minimum of immobilization.
It can take up to six months to return to normal function.
Returning To Normal Activities
After a grade 1 turf toe injury, individuals can return to normal activities once the pain is under control. Grades 2 and 3 take longer to heal. Returning to sports activities after a grade 2 injury can take around two or three months, while grade 3 injuries and cases that require surgery can take up to six months. (Ali-Asgar Najefi et al., 2018)
Sports Chiropractic Treatment
References
American Academy of Orthopaedic Surgeons. (2021). Turf toe.
American College of Foot and Ankle Surgeons. Foot Health Facts. (2023). RICE protocol.
Najefi, A. A., Jeyaseelan, L., & Welck, M. (2018). Turf toe: A clinical update. EFORT open reviews, 3(9), 501–506. doi.org/10.1302/2058-5241.3.180012
Pinter, Z. W., Farnell, C. G., Huntley, S., Patel, H. A., Peng, J., McMurtrie, J., Ray, J. L., Naranje, S., & Shah, A. B. (2020). Outcomes of Chronic Turf Toe Repair in Non-athlete Population: A Retrospective Study. Indian journal of orthopaedics, 54(1), 43–48. doi.org/10.1007/s43465-019-00010-8
Chinn, L., & Hertel, J. (2010). Rehabilitation of ankle and foot injuries in athletes. Clinics in sports medicine, 29(1), 157–167. doi.org/10.1016/j.csm.2009.09.006
When a groin strain injury happens, can knowing the symptoms help in the diagnosis, treatment, and recovery times?
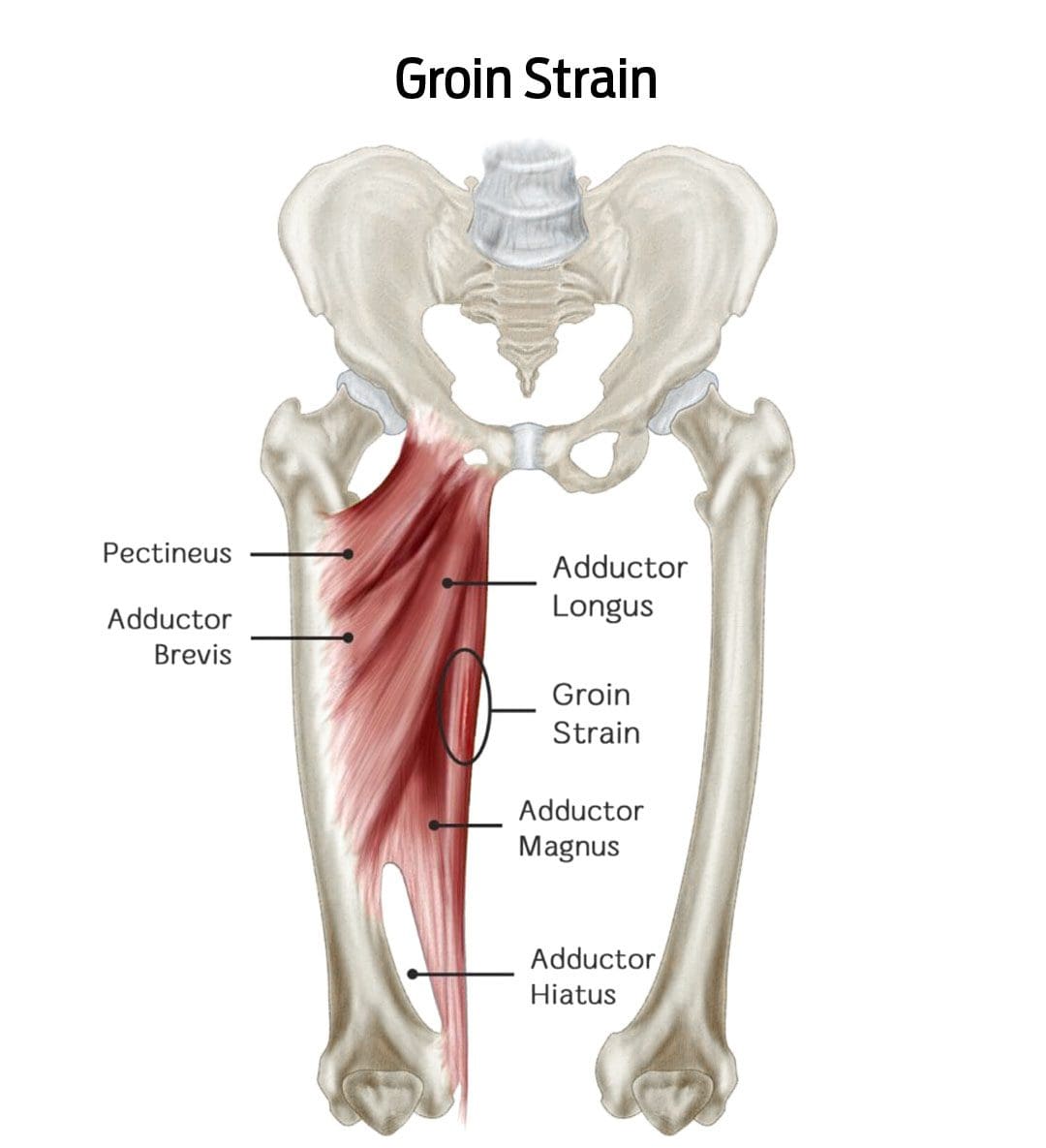
Groin Strain Injury
A groin strain is an injury to an inner thigh muscle. A groin pull is a type of muscle strain affecting the adductor muscle group (the muscles help pull the legs apart). (Parisa Sedaghati, et al., 2013) The injury is caused when the muscle is stretched beyond its normal range of motion, creating superficial tears. Severe strains can tear the muscle in two. (Parisa Sedaghati, et al., 2013)
A groin muscle pull causes pain and tenderness that worsens when squeezing the legs together.
There may also be swelling or bruising in the groin or inner thigh.
An uncomplicated groin pull takes four to six weeks to heal with proper treatment. (Andreas Serner, et al., 2020)
Symptoms
A groin pull can be painful, interfering with walking, navigating stairs, and/or driving a car. In addition to pain, other symptoms around the injured area include: (Parisa Sedaghati et al., 2013)
A popping sound or snapping sensation when the injury occurs.
Increased pain when pulling the legs together.
Redness
Swelling
Bruising of the groin or inner thigh.
Groin pulls are graded by severity and how much they impact mobility:
Grade 1
Mild discomfort but not enough to limit activities.
Grade 2
Moderate discomfort with swelling or bruising that limits running and/or jumping.
Grade 3
Severe injury with significant swelling and bruising can cause pain while walking and muscle spasms.
Signs of a severe groin strain
Difficulty walking
Groin pain while sitting or resting
Groin pain at night
A healthcare provider should see severe groin pulls because the muscle may have ruptured or be on the verge of rupturing.
In severe cases, surgery is necessary to reattach the torn ends.
Groin pulls are sometimes accompanied by a stress fracture of the pubis/forward-facing pelvic bones, which can significantly extend healing and recovery time. (Parisa Sedaghati et al., 2013)
Causes
Groin pulls are often experienced by athletes and individuals who play sports where they must stop and change directions quickly, placing excessive strain on the adductor muscles. (Parisa Sedaghati et al., 2013) The risk is increased in individuals who: (T. Sean Lynch et al., 2017)
Have weak hip abductor muscles.
Are not in adequate physical condition.
Have a previous groin or hip injury.
Pulls can also occur from falls or extreme activities without the proper conditioning.
Diagnosis
A healthcare provider will perform a thorough investigation to confirm the diagnosis and characterize the severity. This involves: (Juan C. Suarez et al., 2013)
Medical History Review
This includes any previous injuries and specifics about where and when the symptoms started.
Physical Examination
This involves palpating – lightly touching and pressing the groin region and manipulating the leg to understand better where and how extensive the injury is.
Imaging Studies
Ultrasound or X-rays.
If a muscle rupture or fracture is suspected, an MRI scan may be ordered to visualize soft tissue injuries and stress fractures better.
Differential Diagnosis
Certain conditions can mimic a groin pull and require different treatments. These include: (Juan C. Suarez, et al., 2013)
Sports Hernia
This type of inguinal hernia occurs with sports and work injuries.
It causes a portion of the intestine to pop through a weakened muscle in the groin.
Hip Labral Tear
This is a tear in the cartilage ring of the labrum outside the rim of the hip joint socket.
Hip Osteoarthritis
This is the wear-and-tear form of arthritis that can present with groin pain symptoms.
Osteitis Pubis
This is inflammation of the pubic joint and surrounding structures, usually caused by the overuse of the hip and leg muscles.
Referred Groin Pain
This nerve pain originates in the lower back, often due to a pinched nerve, but is felt in the groin.
Treatment
Beginning treatment is conservative and includes rest, ice application, physical therapy, and prescribed gentle stretching and exercises.
Individuals may need crutches or a walking device to reduce pain and prevent further injury if the pain is significant. (Andreas Serner, et al., 2020)
Physical therapy will be a part of the treatment plan.
Over-the-counter pain medications like Tylenol/acetaminophen or Advil/ibuprofen can help with pain relief short term.
If there is severe pain from a grade 3 injury, prescription medications may be used for a short period to help minimize pain. (Andreas Serner, et al., 2020)
Sedaghati, P., Alizadeh, M. H., Shirzad, E., & Ardjmand, A. (2013). Review of sport-induced groin injuries. Trauma monthly, 18(3), 107–112. doi.org/10.5812/traumamon.12666
Serner, A., Weir, A., Tol, J. L., Thorborg, K., Lanzinger, S., Otten, R., & Hölmich, P. (2020). Return to Sport After Criteria-Based Rehabilitation of Acute Adductor Injuries in Male Athletes: A Prospective Cohort Study. Orthopaedic journal of sports medicine, 8(1), 2325967119897247. doi.org/10.1177/2325967119897247
Lynch, T. S., Bedi, A., & Larson, C. M. (2017). Athletic Hip Injuries. The Journal of the American Academy of Orthopaedic Surgeons, 25(4), 269–279. doi.org/10.5435/JAAOS-D-16-00171
Suarez, J. C., Ely, E. E., Mutnal, A. B., Figueroa, N. M., Klika, A. K., Patel, P. D., & Barsoum, W. K. (2013). Comprehensive approach to the evaluation of groin pain. The Journal of the American Academy of Orthopaedic Surgeons, 21(9), 558–570. doi.org/10.5435/JAAOS-21-09-558
Individuals who have suffered cervical acceleration-deceleration/CAD more commonly known as whiplash, can experience headaches, and other symptoms like neck stiffness, pain, fatigue, and shoulder/neck/back discomfort. Can non-surgical and conservative treatments help alleviate the symptoms?
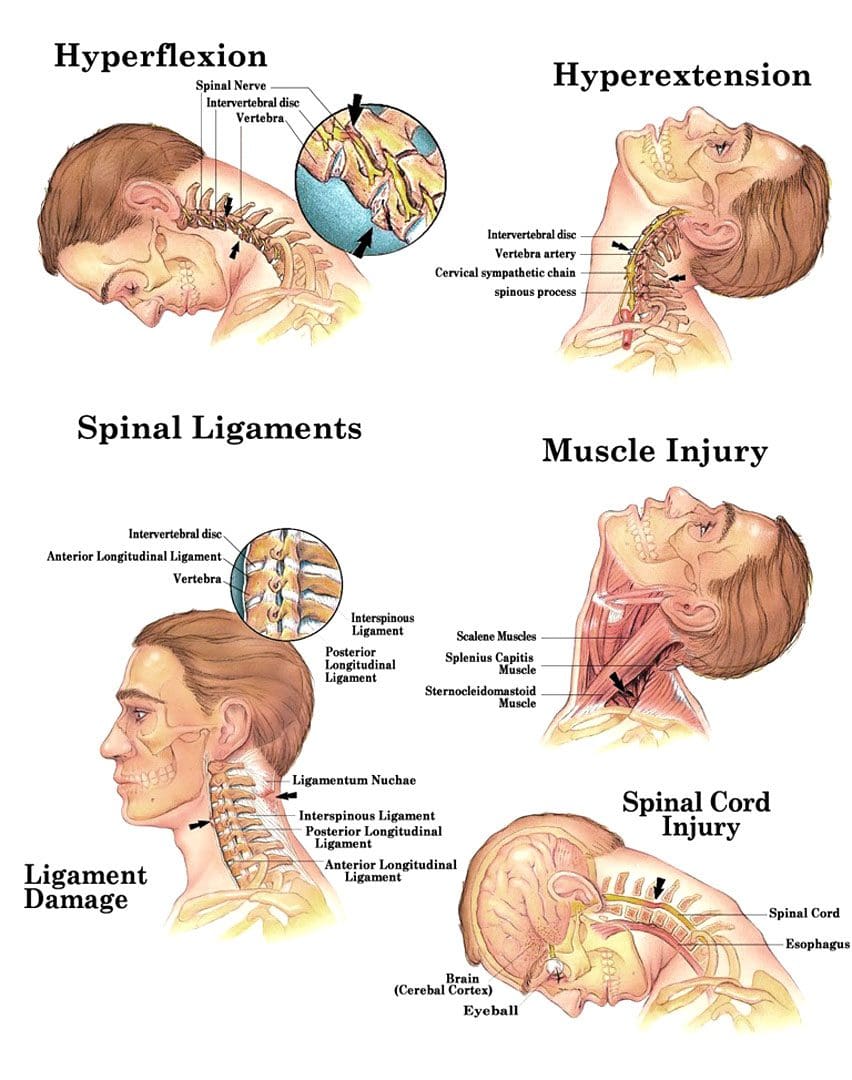
Cervical Acceleration – Deceleration or CAD
Cervical acceleration-deceleration is the mechanism of a neck injury caused by a forceful back-and-forth neck motion. It happens most commonly in rear-end vehicle collisions when the head and neck whip forward and backward with intense acceleration and/or deceleration causing the neck to flex and/or extend rapidly, more than normally, straining and possibly tearing muscle tissues and nerves, ligaments, dislocation of spinal discs and herniations, and cervical bone fractures.
For symptoms that do not improve or worsen after 2 to 3 weeks, see a healthcare provider or chiropractor for further evaluation and treatment.
Whiplash injuries strain or sprain the neck muscles and/or ligaments, but can also affect the vertebrae/bones, disc cushions between the vertebrae, and/or the nerves.
Whiplash symptoms can present right away, or after several hours to a few days after the incident, and tend to worsen in the days after the injury. Symptoms can last a few weeks to a few months, and can severely limit activity and range of motion. Symptoms can include: (National Institute of Neurological Disorders and Stroke. 2023)
Pain that extends into the shoulders and back.
Neck stiffness
Limited neck motion
Muscle spasms
Numbness and tingling sensations – paresthesias or pins and needles in the fingers, hands, or arms.
Headaches – A whiplash headache usually starts at the base of the skull and can vary in intensity. Most individuals experience pain on one side of the head and toward the back, though some can experience symptoms all over their head, and a small number experience headaches on the forehead or behind the eyes. (Monica Drottning. 2003)
The headaches can become aggravated by moving the neck around, especially when looking up.
Headaches are often associated with shoulder pain along with sensitive neck and shoulder muscles that when touched can increase pain levels.
Whiplash headaches can lead to chronic neck-related headaches known as cervicogenic headaches. (Phil Page. 2011)
It is also important to rest your neck area following the injury.
A cervical collar can be utilized temporarily to stabilize the neck, but for long-term recovery, it is recommended to keep the area mobile.
Physical activity reduction until the individual can look over both shoulders, and tilt their head all the way forward, all the way back, and from side to side without pain or stiffness.
Non-steroidal anti-inflammatories – NSAIDs – Ibuprofen or Naproxen.
Muscle relaxers
If symptoms do not improve, a healthcare provider may recommend physical therapy and/or stronger pain medications. For whiplash headaches that last for several months, acupuncture, or spinal injections may be recommended.
Neck Injuries
References
National Institute of Neurological Disorders and Stroke. Whiplash Information Page.
Drottning M. (2003). Cervicogenic headache after a whiplash injury. Current pain and headache reports, 7(5), 384–386. doi.org/10.1007/s11916-003-0038-9
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Temporomandibular joint disorder causes pain and jaw locking that can be worsened with certain activities. How individuals can manage and prevent flare-ups by learning what not to do to worsen the condition?
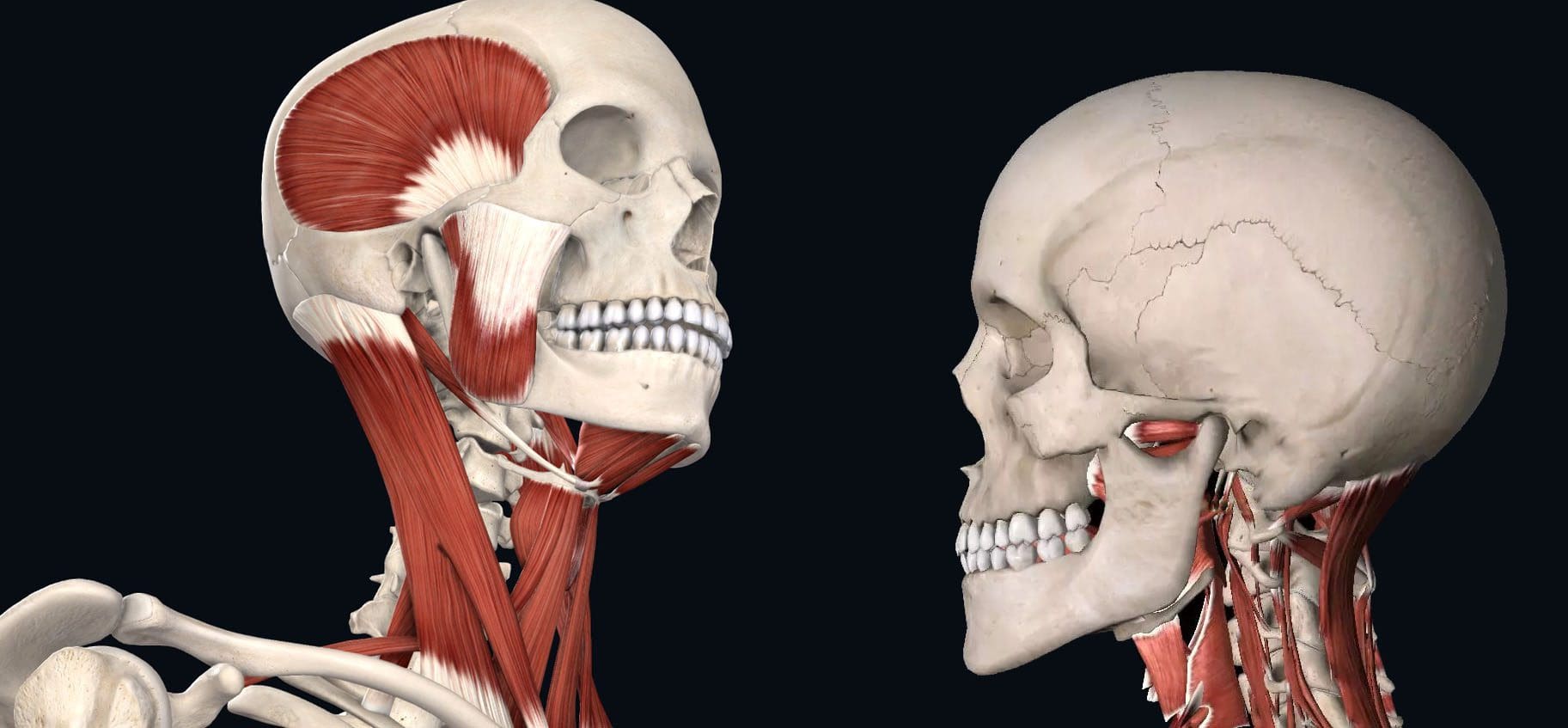
What Not To Do Temporomandibular Joint Disorder
Tenderness, aching, pain, and jaw locking are symptoms of temporomandibular joint disorder or TMJ. The temporomandibular joint connects the jaw to the skull. It is used daily for eating, drinking, and talking. It is a small disc in the joint that allows the jaw bones to slip and slide correctly. With TMJ, the disc shifts out of place, leading to clicking, snapping, and limited jaw movement. It can also cause pain in the jaw and face, neck pain, and headaches, and the muscles around the jaw and neck can become sore and/or go into spasm. Any type of activity that stresses or overworks the joint can trigger a flare-up and worsen TMJ symptoms. (Schiffman E, et al. 2014) This article looks at avoiding activities that make TMJ worse and what not to do to help keep TMJ symptoms in check.
Chewing Gum
Gum chewing is not recommended for individuals with TMJ.
The jaw is one of the most used joints in the body.
Limiting excessive use alleviates pressure allowing the joints and muscles to rest.
Resting sore muscles and joints is the first step in injury recovery.
Eating Chewy and Hard Foods
Chewy and hard foods make the jaw have to work overtime.
Avoid eating hard foods like chewy candies, hard and chewy breads, vegetables like corn on the cob, and fruits like apples.
These foods can place excessive stress on the jaw, and prevent the joint from properly resting and healing.
Chewing Only On One Side
Many individuals chew their food on only one side of the mouth.
This can stress out one side of the temporomandibular joint and surrounding muscles, leading to pain and dysfunction. (Urbano Santana-Mora, et al., 2013)
Stay aware of chewing habits and make sure to utilize both sides of the mouth.
Individuals with dental issues or tooth pain are recommended to see a dentist.
Non-Functional Jaw Activities
Going through each day, individuals tend to do things unconsciously or out of habit.
For example, individuals:
Reading or writing might chew on a pen or pencil.
Bite their nails or chew on the inside of their mouth while watching TV or internet browsing.
These activities can place stress on the joint, worsen the condition, and extend the healing process.
Resting on The Chin
Individuals will rest their jaw in their hands while studying, on social media, or watching TV.
This position can be comfortable, but it can affect the jaw.
This position can build pressure against the side of the jaw and push against the joint, causing the disc to shift out of place affecting how the jaw opens and closes.
Breaking the chin resting habit can allow the joint to relax and heal correctly.
Teeth Clenching
Bruxism is the medical term for clenching the teeth.
This can occur during the day or during sleep.
Teeth clenching is often brought on by stress and can place incredible pressure on the jaw’s muscles and worsen TMJ.
A dentist can prescribe a mouth guard to be worn while sleeping to protect the teeth from excessive clenching. (Miriam Garrigós-Pedrón, et al., 2019)
Slouching
The function of the jaw is closely related to body posture.
The jaw operates optimally when the head is above the cervical spine and the posture is upright.
Slouching can change how the jaw muscles work and the way the jaw opens and closes.
Part of physical therapy for TMJ is working on posture adjustments and training.
This can involve strengthening the back and shoulder muscles and setting up posture reminders.
Sitting and standing correctly can keep the jaw operating properly.
Postponing Treatment
Many with musculoskeletal issues and symptoms wait for the pain to go away.
Individuals having problems with their jaw should not wait to get treatment.
TMJ has a positive rate of recovery with conservative treatment, which is all the more reason to seek treatment. (G Dimitroulis. 2018)
A dentist or healthcare provider can provide an accurate diagnosis if TMJ is suspected.
Individuals can benefit from visiting a physical therapist to learn exercises and strategies to self-treat the condition. (Yasser Khaled, et al., 2017)
Treatment
Treatment can involve:
Initial treatment focuses on pain relief and jaw function opens and closes improvement.
A guard can help with night teeth grinding/bruxism.
Anti-inflammatory treatments.
In severe cases, surgery may be recommended to correct the problem, as a last resort. (Meghan K Murphy, et al., 2013)
Follow recommendations on what not to do and avoid certain activities.
Quick Patient Initiation
References
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., Jensen, R., … Orofacial Pain Special Interest Group, International Association for the Study of Pain (2014). Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. Journal of oral & facial pain and headache, 28(1), 6–27. doi.org/10.11607/jop.1151
Santana-Mora, U., López-Cedrún, J., Mora, M. J., Otero, X. L., & Santana-Penín, U. (2013). Temporomandibular disorders: the habitual chewing side syndrome. PloS one, 8(4), e59980. doi.org/10.1371/journal.pone.0059980
Garrigós-Pedrón, M., Elizagaray-García, I., Domínguez-Gordillo, A. A., Del-Castillo-Pardo-de-Vera, J. L., & Gil-Martínez, A. (2019). Temporomandibular disorders: improving outcomes using a multidisciplinary approach. Journal of multidisciplinary healthcare, 12, 733–747. doi.org/10.2147/JMDH.S178507
Dimitroulis G. (2018). Management of temporomandibular joint disorders: A surgeon’s perspective. Australian Dental Journal, 63 Suppl 1, S79–S90. doi.org/10.1111/adj.12593
Khaled Y, Quach JK, Brennan MT, NapeÑas JJ. Outcomes after physical therapy for the treatment of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017;124(3: e190. doi:10.1016/j.oooo.2017.05.477
Abouelhuda, A. M., Khalifa, A. K., Kim, Y. K., & Hegazy, S. A. (2018). Non-invasive different modalities of treatment for temporomandibular disorders: a review of the literature. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 44(2), 43–51. doi.org/10.5125/jkaoms.2018.44.2.43
Murphy, M. K., MacBarb, R. F., Wong, M. E., & Athanasiou, K. A. (2013). Temporomandibular disorders: a review of etiology, clinical management, and tissue engineering strategies. The International journal of oral & maxillofacial implants, 28(6), e393–e414. doi.org/10.11607/jomi.te20
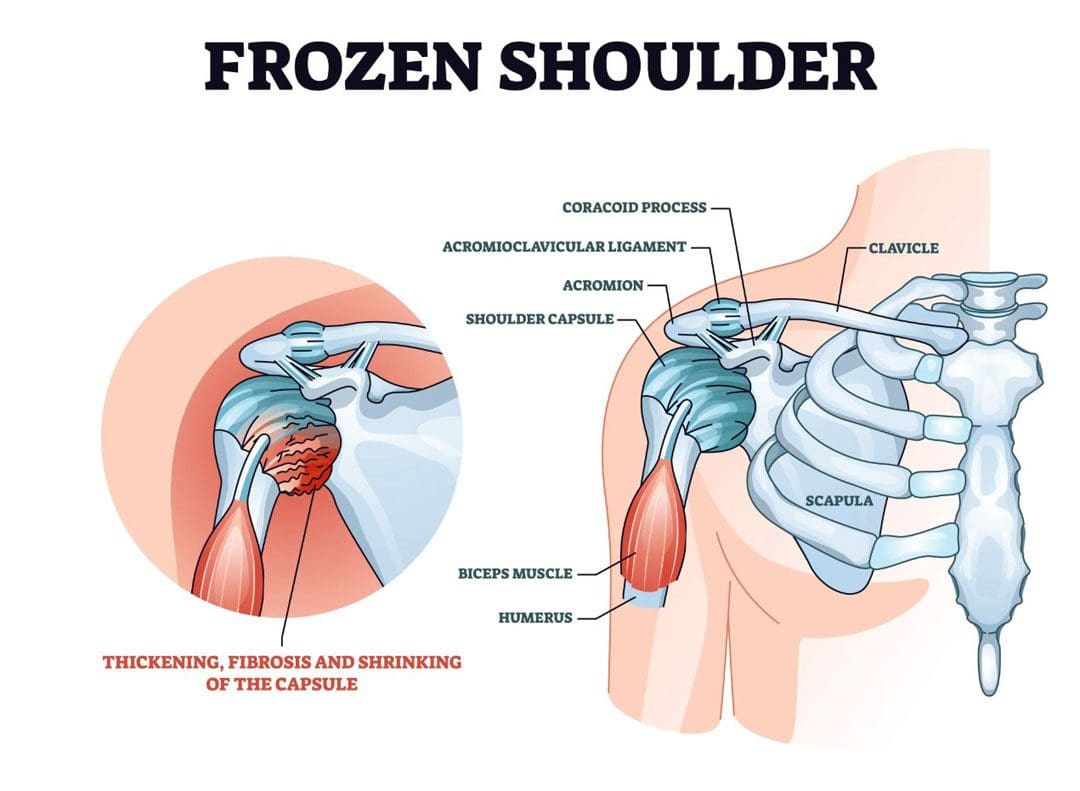
Stiffness and pain developing in the shoulder could be adhesive capsulitis, (frozen shoulder), a condition in the shoulder’s ball-and-socket joint/glenohumeral joint. It usually develops over time and limits the functional use of the arm. The pain and tightness restrict arm movement, and the duration of symptoms can persist for 12-18 months. The cause is often unknown, but it is more common in individuals over 40, individuals with diabetes, thyroid disease, and cardiac conditions have an increased risk of developing the condition, and women tend to develop the condition more than men. Chiropractic treatment can be effective at relieving pain and expediting recovery.
Stiffness and Pain
The shoulder joint allows more movement than any other joint in the body. A frozen shoulder causes the capsule surrounding the shoulder joint to contract and form scar tissue. The capsule contraction and the formation of adhesions cause the shoulder to become stiff, restrict movement, and cause pain and discomfort symptoms.
Stages
The progression is marked by three stages:
Freezing
Stiffness and pain begin to restrict motion.
Frozen
Movement and motion are severely restricted.
Thawing
The shoulder starts to loosen up.
It can take years to fully resolve symptoms.
In mild cases, a frozen shoulder can go away on its own but that does not mean that it is truly healed and correctly aligned.
Even in mild cases seeking treatment is recommended, rather than just waiting for it to go away.
Symptoms
Limited range of motion.
Stiffness and tightness.
Dull or aching pain throughout the shoulder.
Pain can radiate into the upper arm.
Pain can be triggered by the smallest movements.
The symptoms are not always due to weakness or injury, but actual joint stiffness.
Causes
Most frozen shoulders occur with no injury or discernible cause but the condition is often linked to a systemic condition or one that affects the entire body.
Age and Gender
Frozen shoulder most commonly affects individuals between the ages of 40 to 60, and is more common in women than in men.
Endocrine Disorders
Individuals with diabetes have an increased risk of developing a frozen shoulder.
Other endocrine abnormalities like thyroid problems can also lead to the development of this condition.
Shoulder Trauma and/or Surgery
Individuals who sustain a shoulder injury, or undergo surgery on the shoulder can develop a stiff and painful joint.
When injury or surgery is followed by prolonged immobilization/resting the arm, the risk of developing a frozen shoulder increases.
Other Systemic Conditions
Several systemic conditions such as heart disease have also been associated with an increased risk of developing the condition and can include:
High cholesterol
Adrenal disease
Heart and lung disease
Parkinson’s disease
Stiffness and pain can also be associated with damage to the joint from injuries or other shoulder problems that include:
A frozen shoulder associated with any of these causes is considered secondary.
Treatment
A diagnosis is made by observing the range of motion in the shoulder, considering the two types:
Active Range
This is how far an individual can move a body part on their own.
Passive Range
This is how far another person like a therapist or doctor can move the body part.
Therapies
Chiropractic, massage, and physical therapy involve stretches, realignment, and exercises to relieve pain symptoms and restore mobility and function.
Usually, strength is not affected by a frozen shoulder but a chiropractor may want to strengthen the surrounding muscles to better support the shoulder and prevent worsening the injury or causing a new injury.
Anti-inflammatory medications and corticosteroid injections may help manage pain symptoms.
Getting a diagnosis and treatment during the freezing stage can keep the condition from progressing and expedite recovery time.
Enhancing Health: Evaluation and Treatment
References
Brun, Shane. “Idiopathic frozen shoulder.” Australian Journal of general practice vol. 48,11 (2019): 757-761. doi:10.31128/AJGP-07-19-4992
Chan, Hui Bin Yvonne, et al. “Physical therapy in the management of frozen shoulder.” Singapore medical journal vol. 58,12 (2017): 685-689. doi:10.11622/smedj.2017107
Cho, Chul-Hyun, et al. “Treatment Strategy for Frozen Shoulder.” Clinics in orthopedic surgery vol. 11,3 (2019): 249-257. doi:10.4055/cios.2019.11.3.249
Duzgun, Irem, et al. “Which method for frozen shoulder mobilization: manual posterior capsule stretching or scapular mobilization?.” Journal of Musculoskeletal & neuronal interactions vol. 19,3 (2019): 311-316.
Jain, Tarang K, and Neena K Sharma. “The effectiveness of physiotherapeutic interventions in the treatment of frozen shoulder/adhesive capsulitis: a systematic review.” Journal of back and musculoskeletal rehabilitation vol. 27,3 (2014): 247-73. doi:10.3233/BMR-130443
Kim, Min-Su, et al. “Diagnosis and treatment of calcific tendinitis of the shoulder.” Clinics in shoulder and elbow vol. 23,4 210-216. 27 Nov. 2020, doi:10.5397/cise.2020.00318
Millar, Neal L et al. “Frozen shoulder.” Nature reviews. Disease primers vol. 8,1 59. 8 Sep. 2022, doi:10.1038/s41572-022-00386-2
Massage guns can help relieve aching muscles and prevent soreness when used before and after physical activity, work, school, and exercise. They provide massage therapy benefits by targeting muscles with rapid burst pulses. Massage guns can be percussive or vibration-based. Percussive therapy helps increase blood flow to a targeted area, which reduces inflammation and muscle tension, and breaks up knots/trigger points that may have formed in the tissues from added stress or intense physical activity. One of the benefits is that they come with interchangeable massage gun head attachments that target different muscle groups and provide different types of massage. There are many types of interchangeable massage heads, we go over the most common to give a general idea of how they work. If experiencing joint pain, injury, acute muscle pain, or other musculoskeletal disorders, make sure to get clearance from a doctor before using a massage gun.
Massage Gun Head Attachments
The variations of attachments/heads are designed and shaped differently to effectively apply the right amount of pressure to rejuvenate the body’s pressure points, soothe tissues, and release tight and sore muscles. The different heads are designed with a distinctive purpose based on the muscle groups targeted. This maximizes effectiveness and ensures maximum comfort and safety.
Ball Head
The ball attachment is for overall muscle recovery.
It provides a broad surface area and mimics the hands of a skilled massage therapist, delivering a soothing kneading sensation.
Made of durable material, the ball massage head can reach deep into the muscles.
Its round shape makes it more flexible to use anywhere, especially the large muscle groups like the quads and glutes.
U/Fork Shaped Head
A plastic, dual-pronged head also known as a fork head.
The attachment provides relief to areas like the shoulders, spine, neck, calves, and Achilles tendon.
Bullet Head
The plastic head is named as such because of its pointed shape.
This is recommended for tightness and discomfort in the joints, deep tissues, trigger points, and/or small muscle areas like the feet and wrist.
Flat Head
The multipurpose flat head is for full-body general massage.
It helps relieve stiffness and pain for total body muscle relaxation, including muscle groups closer to bone joints.
Shovel-Shaped Head
The shovel-shaped head is for the abdominal muscles and lower back.
The attachment provides stimulation to release stiff muscles.
Using The Right Head
Which head to use depends on the individual’s specific needs and preferences. Consider the following factors when selecting a massage gun head:
Targeted Areas
Identify the body areas requiring the most attention.
If muscle tightness or soreness is occurring in larger muscle groups, like the back or legs, the ball attachment is recommended.
For more precise areas like trigger points, the bullet head is recommended.
Heads can be used in conjunction – for example, a large surface area head is used to relax and loosen and relax a general area, then a more precise head is used to focus the massage on the actual tight spot or trigger point.
Massage Intensity
Massage intensity levels can be varied from a light massage to full force.
For a softer touch on sensitive muscles, flat head or forkhead attachments are recommended.
For deep muscle penetration and consistent pressure, the bullet head or shovel head attachments are recommended.
Specific Conditions
Consider any specific conditions or injuries previous and current.
For individuals recovering from an injury or with sensitive areas, it’s important to choose a massage gun head that provides the necessary relief without causing discomfort or worsening an injury.
Try Out Different Heads and Settings
Experiment with different massage head attachments and speeds to find the one that works best for the intended purpose.
Explore each to discover personal preferences.
Start with the lowest setting and gradually increase, based on comfort level.
Always consult with a qualified healthcare provider regarding any medical concerns before using a massage gun.
Choosing The Right Massage Head Attachment
References
Bergh, Anna, et al. “A Systematic Review of Complementary and Alternative Veterinary Medicine in Sport and Companion Animals: Soft Tissue Mobilization.” Animals: an open access journal from MDPI vol. 12,11 1440. 2 Jun. 2022, doi:10.3390/ani12111440
Imtiyaz, Shagufta, et al. “To Compare the Effect of Vibration Therapy and Massage in Prevention of Delayed Onset Muscle Soreness (DOMS).” Journal of Clinical and diagnostic research: JCDR vol. 8,1 (2014): 133-6. doi:10.7860/JCDR/2014/7294.3971
Konrad, Andreas, et al. “The Acute Effects of a Percussive Massage Treatment with a Hypervolt Device on Plantar Flexor Muscles’ Range of Motion and Performance.” Journal of sports science & medicine vol. 19,4 690-694. 19 Nov. 2020
Leabeater, Alana et al. “Under the Gun: The effect of percussive massage therapy on physical and perceptual recovery in active adults.” Journal of athletic training, 10.4085/1062-6050-0041.23. 26 May. 2023, doi:10.4085/1062-6050-0041.23
Lupowitz, Lewis. “Vibration Therapy – A Clinical Commentary.” International journal of sports physical therapy vol. 17,6 984-987. 1 Aug. 2022, doi:10.26603/001c.36964
Yin, Yikun, et al. “The effect of vibration training on delayed muscle soreness: A meta-analysis.” Medicine vol. 101,42 (2022): e31259. doi:10.1097/MD.0000000000031259
Overexertion and repetitive stress injuries make up a fourth of all work injuries. Repetitive pulling, lifting, punching in numbers, typing, pushing, holding, carrying, and scanning are the most common causes of job-related injuries. These types of injuries are the most common that cause missed days at work. Overexertion can lead to lasting physical chronic conditions, ranging from chronic back pain to chronic joint pain caused by the advanced wearing and tearing of the various musculoskeletal tissues. Chiropractic medicine takes a comprehensive and whole-body approach to treating neuromusculoskeletal injuries. Chiropractic relieves tight or damaged muscles, increases nerve energy flow, and properly aligns the joints through adjustments, spinal traction, decompression, and various forms of manual manipulation.
Overexertion and Repetitive Stress Injuries
Overexertion and repetitive stress injuries typically occur over time/years of engaging in the same strenuous activity regularly. However, an overexertion injury can occur with one sudden or extreme movement. A worker can injure muscles, tendons, joints, and ligaments. Overexertion can lead to musculoskeletal disorders with symptoms including:
Inflammation
Swelling
Numbness
Stiffness
Chronic pain
Limited or total loss of mobility in the muscles, tendons, ligaments, and joints.
Types
A few of the most common examples of overexertion injuries include:
Soft-Tissue
Injuries to muscles, ligaments, tendons, and joints.
Back
Pulled, strained back muscles.
Herniated discs.
Compressed nerve roots.
Fractured vertebrae.
Dehydration and Heat Stroke
Most common among workers doing outdoor manual labor.
Repetitive and Overuse
Injuries range from carpal tunnel syndrome to stress fractures.
Often the result of weeks, months, or years of repeated movements
In many cases, two or more injuries can happen simultaneously.
For example, a worker is more likely to sustain an injury if they are dehydrated or they are performing dual tasks.
Causes
Certain movements and activities are more likely to cause overexertion injuries. Some of the most common include:
Daily lifting of objects, light and heavy.
Performing awkward movements that cause the body to be in unhealthy positions.
Standing and/or sitting or for long periods.
Using excessive force to perform tasks.
Operating heavy machinery.
Working in hot and/or humid conditions.
High-Rate Injury Industries
Industries in which overexertion injuries are most common include:
Education.
Health services.
Manufacturing.
Construction.
Warehouse work.
Transportation.
Wholesale trade.
Retail stores.
Chiropractic Treatment
These injuries can lead to missed work, debilitating pain, and medical bills. Depending on the severity of the injury, chiropractic care will use massage techniques, spinal manipulation, traction, and decompression therapies, to increase flexibility and mobility to reduce the chances of a recurring injury. The benefits of chiropractic include:
Prevents the risk of worsening or future injuries.
Expedites recovery to help individuals rehabilitate and get back to work sooner.
Improves physical and mental well-being.
Provide recommendations on how to properly stretch and strengthen muscles.
Nutritional anti-inflammatory recommendations.
By learning how to avoid overexertion injuries, workers can be more productive, enjoy work, and improve their quality of life.
From Injury To Recovery
References
Anderson, Vern Putz, et al. “Occupational fatalities, injuries, illnesses, and related economic loss in the wholesale and retail trade sector.” American Journal of industrial medicine vol. 53,7 (2010): 673-85. doi:10.1002/ajim.20813
Choi, Hyun-Woo, et al. “Characteristics of occupational musculoskeletal disorders of five sectors in the service industry between 2004 and 2013.” Annals of Occupational and environmental medicine vol. 29 41. 19 Sep. 2017, doi:10.1186/s40557-017-0198-4
Friedenberg, Rivi, et al. “Work-related musculoskeletal disorders and injuries among emergency medical technicians and paramedics: A comprehensive narrative review.” Archives of Environmental & occupational health vol. 77,1 (2022): 9-17. doi:10.1080/19338244.2020.1832038
Galinsky, T et al. “Overexertion injuries in home health care workers and the need for ergonomics.” Home health care services quarterly vol. 20,3 (2001): 57-73. doi:10.1300/J027v20n03_04
González Fuentes, Aroa, et al. “Work-related overexertion injuries in cleaning occupations: An exploration of the factors to predict the days of absence by means of machine learning methodologies.” Applied ergonomics, vol. 105 103847. 30 Jul. 2022, doi:10.1016/j.apergo.2022.103847
Schoenfisch, Ashley L et al. “Declining rates of work-related overexertion back injuries among union drywall installers in Washington State, 1989-2008: Improved work safety or shifting of care?.” American Journal of industrial medicine vol. 57,2 (2014): 184-94. doi:10.1002/ajim.22240
Williams, J M et al. “Work-related injuries in a rural emergency department population.” Academic emergency medicine: official journal of the Society for Academic Emergency Medicine vol. 4,4 (1997): 277-81. doi:10.1111/j.1553-2712.1997.tb03548.x
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine