Back Clinic Nerve Injury Team. Nerves are fragile and can be damaged by pressure, stretching, or cutting. Injury to a nerve can stop signals to and from the brain, causing muscles not to work properly and losing feeling in the injured area. The nervous system manages a great majority of the body’s functions, from regulating an individual’s breathing to controlling their muscles as well as sensing heat and cold. But, when trauma from an injury or an underlying condition causes nerve injury, an individual’s quality of life may be greatly affected. Dr. Alex Jimenez explains various concepts through his collection of archives revolving around the types of injuries and condition which can cause nerve complications as well as discuss the different form of treatments and solutions to ease nerve pain and restore the individual’s quality of life.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
When sciatica or other radiating nerve pain presents, can learning to distinguish between nerve pain and different types of pain help individuals recognize when spinal nerve roots are irritated or compressed or more serious problems that require medical attention?
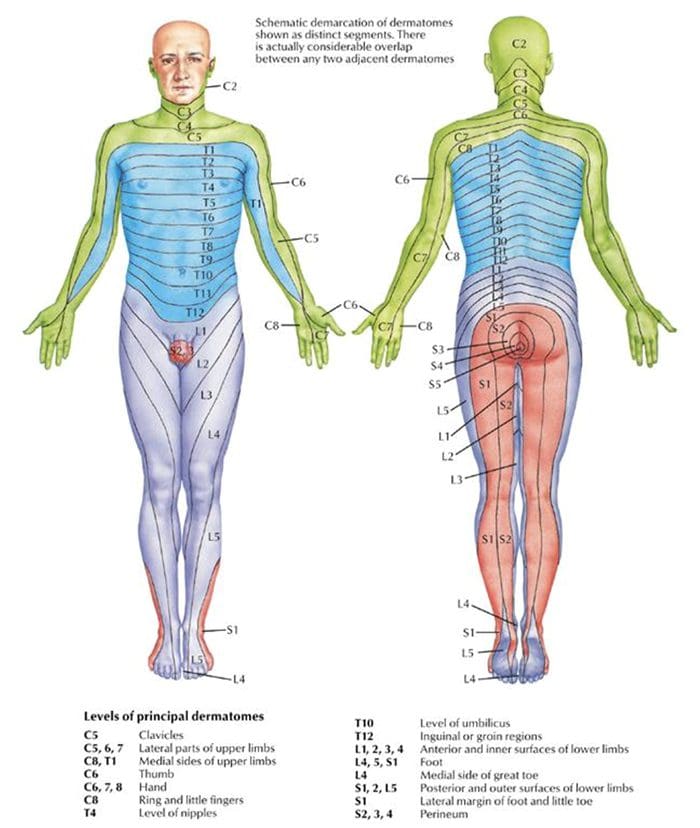
Spinal Nerve Roots and Dermatomes
Spinal conditions such as herniated discs and stenosis can lead to radiating pain that travels down one arm or leg. Other symptoms include weakness, numbness, and/or shooting or burning electrical sensations. The medical term for pinched nerve symptoms is radiculopathy (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020). Dermatomes could contribute to irritation in the spinal cord, where the nerve roots cause symptoms in the back and limbs.
Anatomy
The spinal cord has 31 segments.
Each segment has nerve roots on the right and left that supply motor and sensory functions to the limbs.
The anterior and posterior communicating branches combine to form the spinal nerves that exit the vertebral canal.
The 31 spine segments result in 31 spinal nerves.
Each one transmits sensory nerve input from a specific skin region on that side and area of the body.
These regions are called dermatomes.
Except for the first cervical spinal nerve, dermatomes exist for each spinal nerve.
The spinal nerves and their associated dermatomes form a network all over the body.
Dermatomes Purpose
Dermatomes are the body/skin areas with sensory input assigned to individual spinal nerves. Each nerve root has an associated dermatome, and various branches supply each dermatome off that single nerve root. Dermatomes are pathways through which sensational information in the skin transmits signals to and from the central nervous system. Sensations that are physically felt, like pressure and temperature, get transmitted to the central nervous system. When a spinal nerve root becomes compressed or irritated, usually because it comes into contact with another structure, it results in radiculopathy. (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020).
Radiculopathy
Radiculopathy describes symptoms caused by a pinched nerve along the spine. Symptoms and sensations depend on where the nerve is pinched and the extent of the compression.
Cervical
This is a syndrome of pain and/or sensorimotor deficiencies when nerve roots in the neck are compressed.
It often presents with pain that goes down one arm.
Individuals may also experience electrical sensations like pins and needles, shocks, and burning sensations, as well as motor symptoms like weakness and numbness.
Lumbar
This radiculopathy results from compression, inflammation, or injury to a spinal nerve in the lower back.
Sensations of pain, numbness, tingling, electrical or burning sensations, and motor symptoms like weakness traveling down one leg are common.
Diagnosis
Part of a radiculopathy physical examination is testing the dermatomes for sensation. The practitioner will use specific manual tests to determine the spinal level from which the symptoms originate. Manual exams are often accompanied by diagnostic imaging tests like MRI, which can show abnormalities in the spinal nerve root. A complete physical examination will determine if the spinal nerve root is the source of the symptoms.
Treating Underlying Causes
Many back disorders can be treated with conservative therapies to provide effective pain relief. For a herniated disk, for example, individuals may be recommended to rest and take a nonsteroidal anti-inflammatory medication. Acupuncture, physical therapy, chiropractic, non-surgical traction, or decompression therapies may also be prescribed. For severe pain, individuals may be offered an epidural steroid injection that can provide pain relief by reducing inflammation. (American Academy of Orthopaedic Surgeons: OrthoInfo. 2022) For spinal stenosis, a provider may first focus on physical therapy to improve overall fitness, strengthen the abdominals and back muscles, and preserve motion in the spine. Pain-relieving medications, including NSAIDs and corticosteroid injections, can reduce inflammation and relieve pain. (American College of Rheumatology. 2023) Physical therapists provide various therapies to decrease symptoms, including manual and mechanical decompression and traction. Surgery may be recommended for cases of radiculopathy that don’t respond to conservative treatments.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility, and mobility Fitness Training, and Rehabilitation Systems for all ages. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers to bring El Paso, the top clinical treatments, to our community.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery
Individuals experiencing shooting, aching pain in the lower extremities, and intermittent leg pain could be suffering from neurogenic claudication. Can knowing the symptoms help healthcare providers develop an effective treatment plan?
Neurogenic Claudication
Neurogenic claudication occurs when spinal nerves become compressed in the lumbar or lower spine, causing intermittent leg pain. Compressed nerves in the lumbar spine can cause leg pain and cramps. The pain usually worsens with specific movements or activities like sitting, standing, or bending backward. It is also known as pseudo-claudication when the space within the lumbar spine narrows. A condition known as lumbar spinal stenosis. However, neurogenic claudication is a syndrome or group of symptoms caused by a pinched spinal nerve, while spinal stenosis describes the narrowing of the spinal passages.
Symptoms
Neurogenic claudication symptoms can include:
Leg cramping.
Numbness, tingling, or burning sensations.
Leg fatigue and weakness.
A sensation of heaviness in the leg/s.
Sharp, shooting, or aching pain extending into the lower extremities, often in both legs.
There may also be pain in the lower back or buttocks.
Neurogenic claudication is different from other types of leg pain, as the pain alternates – ceasing and beginning randomly and worsens with specific movements or activities. Standing, walking, descending stairs, or flexing backward can trigger pain, while sitting, climbing stairs, or leaning forward tends to relieve pain. However, every case is different. Over time, neurogenic claudication can affect mobility as individuals try to avoid activities that cause pain, including exercise, lifting objects, and prolonged walking. In severe cases, neurogenic claudication can make sleeping difficult.
Neurogenic claudication and sciatica are not the same. Neurogenic claudication involves nerve compression in the central canal of the lumbar spine, causing pain in both legs. Sciatica involves compression of nerve roots exiting from the sides of the lumbar spine, causing pain in one leg. (Carlo Ammendolia, 2014)
Causes
With neurogenic claudication, compressed spinal nerves are the underlying cause of the leg pain. In many cases, lumber spinal stenosis – LSS is the cause of pinched nerve. There are two types of lumbar spinal stenosis.
Central stenosis is the main cause of neurogenic claudication. With this type, the central canal of the lumbar spine, which houses the spinal cord, narrows, causing pain in both legs.
Lumbar spinal stenosis can be acquired and develop later in life due to spine deterioration.
Congenital means the individual is born with the condition.
Both can lead to neurogenic claudication in different ways.
Foramen stenosis is another type of lumbar spinal stenosis that causes the narrowing of spaces on either side of the lumbar spine where nerve roots branch off the spinal cord. The associated pain is different in that it is either in the right or left leg.
The pain corresponds to the side of the spinal cord where the nerves are being pinched.
Acquired Lumbar Spinal Stenosis
Lumbar spinal stenosis is usually acquired due to the degeneration of the lumbar spine and tends to affect older adults. The causes of the narrowing can include:
Spinal trauma, such as from a vehicle collision, work, or sports injury.
Disc herniation.
Spinal osteoporosis – wear-and-tear arthritis.
Ankylosing spondylitis – a type of inflammatory arthritis that affects the spine.
Osteophytes – bone spurs.
Spinal tumors – non-cancerous and cancerous tumors.
Congenital Lumbar Spinal Stenosis
Congenital lumbar spinal stenosis means an individual is born with abnormalities of the spine that may not be apparent at birth. Because the space within the spinal canal is already narrow, the spinal cord is vulnerable to any changes as the individual ages. Even individuals with mild arthritis can experience symptoms of neurogenic claudication early on and develop symptoms in their 30s and 40s instead of their 60s and 70s.
Diagnosis
Diagnosis of neurogenic claudication is largely based on the individual’s medical history, physical examination, and imaging. The physical examination and review identify where the pain is presenting and when. The healthcare provider may ask:
Is there a history of lower back pain?
Is the pain in one leg or both?
Is the pain constant?
Does the pain come and go?
Does the pain get better or worse when standing or sitting?
Do movements or activities cause pain symptoms and sensations?
Are there any usual sensations while walking?
Treatment
Treatments can consist of physical therapy, spinal steroid injections, and pain meds. Surgery is a last resort when all other therapies are unable to provide effective relief.
Physical Therapy
A treatment plan will involve physical therapy that includes:
Daily stretching
Strengthening
Aerobic exercises
This will help improve and stabilize the lower back muscles and correct posture problems.
Occupational therapy will recommend activity modifications that cause pain symptoms.
This includes proper body mechanics, energy conservation, and recognizing pain signals.
Back braces or belts may also be recommended.
Spinal Steroid Injections
Healthcare providers may recommend epidural steroid injections.
This delivers a cortisone steroid to the outermost section of the spinal column or the epidural space.
Pain medications are used to treat intermittent neurogenic claudication. These include:
Over-the-counter analgesics like acetaminophen.
Nonsteroidal anti-inflammatory drugs or NSAIDs like ibuprofen or naproxen.
Prescription NSAIDs may be prescribed if needed.
NSAIDs are used with chronic neurogenic pain and should only be used when required.
The long-term use of NSAIDs can increase the risk of stomach ulcers, and the overuse of acetaminophen can lead to liver toxicity and liver failure.
Surgery
If conservative treatments are unable to provide effective relief and mobility and/or quality of life are affected, surgery known as a laminectomy may be recommended to decompress the lumbar spine. The procedure may be performed:
Laparoscopically – with small incisions, scopes, and surgical instrumentation.
Open surgery – with a scalpel and sutures.
During the procedure, facets of the vertebra are partially or completely removed.
To provide stability, the bones are sometimes fused with screws, plates, or rods.
Success rates for both are more or less the same.
Between 85% and 90% of individuals undergoing the surgery achieve long-lasting and/or permanent pain relief. (Xin-Long Ma et al., 2017)
Movement Medicine: Chiropractic Care
References
Ammendolia C. (2014). Degenerative lumbar spinal stenosis and its imposters: three case studies. The Journal of the Canadian Chiropractic Association, 58(3), 312–319.
Munakomi S, Foris LA, Varacallo M. (2024). Spinal Stenosis and Neurogenic Claudication. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK430872/
Ma, X. L., Zhao, X. W., Ma, J. X., Li, F., Wang, Y., & Lu, B. (2017). Effectiveness of surgery versus conservative treatment for lumbar spinal stenosis: A system review and meta-analysis of randomized controlled trials. International journal of surgery (London, England), 44, 329–338. doi.org/10.1016/j.ijsu.2017.07.032
For individuals dealing with chronic pain, can undergoing a nerve block procedure help alleviate and manage symptoms?
Nerve Blocks
A nerve block is a procedure done to interrupt/block pain signals due to nerve dysfunction or injury. They can be used for diagnostic or treatment purposes, and their effects can be short or long-term, depending on the type being used.
A temporary nerve block may involve the application or injection that stops pain signals from transmitting for a short time.
For example, in pregnancy, an epidural injection can be used during labor and delivery.
Permanent nerve blocks involve cutting/severing or removing certain parts of a nerve to stop pain signals.
These are used in cases with severe injuries or other chronic pain conditions that have not improved with other treatment approaches.
Treatment Usage
When healthcare providers diagnose a chronic pain condition caused by nerve injury or dysfunction, they may use a nerve block to locate the area generating pain signals. They may perform electromyography and/or a nerve conduction velocity/NCV test to pinpoint the cause of chronic nerve pain. Nerve blocks can also treat chronic neuropathic pain, such as pain caused by nerve damage or compression. Nerve blocks are regularly used to treat back and neck pain caused by herniated discs or spinal stenosis. (Johns Hopkins Medicine. 2024)
Types
Three types include:
Local
Neurolytic
Surgical
All three can be used for conditions that cause chronic pain. However, neurolytic and surgical blocks are permanent and are only used for severe pain that has worsened with other treatments unable to provide relief.
Temporary Blocks
A local block is done by injecting or applying local anesthetics, like lidocaine, to a certain area.
An epidural is a local nerve block that injects steroids or analgesics into an area around the spinal cord.
These are common during pregnancy, labor, and delivery.
Epidurals can also be used to treat chronic neck or back pain due to a compressed spinal nerve.
Local blocks are usually temporary, but in a treatment plan, they can be repeated over time to manage chronic pain from conditions like arthritis, sciatica, and migraines. (NYU Langone Health. 2023)
Permanent Blocks
A neurolytic block uses alcohol, phenol, or thermal agents to treat chronic nerve pain. (National Institute of Neurological Disorders and Stroke. 2023) These procedures damage certain areas of the nerve pathway on purpose so that pain signals cannot be transmitted. A neurolytic block is mainly used for severe chronic pain cases, like pain from cancer or complex regional pain syndrome/CRPS. They are sometimes used to treat ongoing pain from chronic pancreatitis and pain in the chest wall after surgery. (Johns Hopkins Medicine. 2024) (Alberto M. Cappellari et al., 2018)
The neurosurgeon performs a surgical nerve block that involves surgically removing or damaging specific areas of the nerve. (National Institute of Neurological Disorders and Stroke. 2023) A surgical nerve block is only used for severe pain cases, such as cancer pain or trigeminal neuralgia.
Although neurolytic and surgical nerve blocks are permanent procedures, pain symptoms, and sensations can come back if the nerves are able to regrow and repair themselves. (Eun Ji Choi et al., 2016) However, symptoms and sensations may not return months or years after the procedure.
These procedures can have the potential risk of permanent nerve damage. (Anthem BlueCross. 2023) Nerves are sensitive and regenerate slowly, so a tiny error can cause side effects. (D O’Flaherty et al., 2018) Common side effects include:
Muscle paralysis
Weakness
Frequent numbness
In rare cases, the block could irritate the nerve and cause added pain.
Skilled and licensed health practitioners like surgeons, pain management physicians, anesthesiologists, and dentists are trained to perform these procedures carefully.
There is always a risk of nerve damage or injury, but the majority of nerve blocks safely and successfully decrease and help manage chronic pain. (Anthem BlueCross. 2023)
What to Expect
Individuals may feel numbness or soreness and/or notice redness or irritation near or around the area that is temporary.
There can also be swelling, which compresses the nerve and requires time to improve. (Stanford Medicine. 2024)
Individuals may be asked to rest for a certain amount of time after the procedure.
Depending on the type of procedure, individuals may have to spend a few days in a hospital.
Some pain may still be present, but that does not mean the procedure did not work.
Individuals should consult with a healthcare provider about the risks and benefits to ensure it is the right treatment.
Cappellari, A. M., Tiberio, F., Alicandro, G., Spagnoli, D., & Grimoldi, N. (2018). Intercostal Neurolysis for The Treatment of Postsurgical Thoracic Pain: a Case Series. Muscle & nerve, 58(5), 671–675. doi.org/10.1002/mus.26298
Choi, E. J., Choi, Y. M., Jang, E. J., Kim, J. Y., Kim, T. K., & Kim, K. H. (2016). Neural Ablation and Regeneration in Pain Practice. The Korean journal of pain, 29(1), 3–11. doi.org/10.3344/kjp.2016.29.1.3
O’Flaherty, D., McCartney, C. J. L., & Ng, S. C. (2018). Nerve injury after peripheral nerve blockade-current understanding and guidelines. BJA education, 18(12), 384–390. doi.org/10.1016/j.bjae.2018.09.004
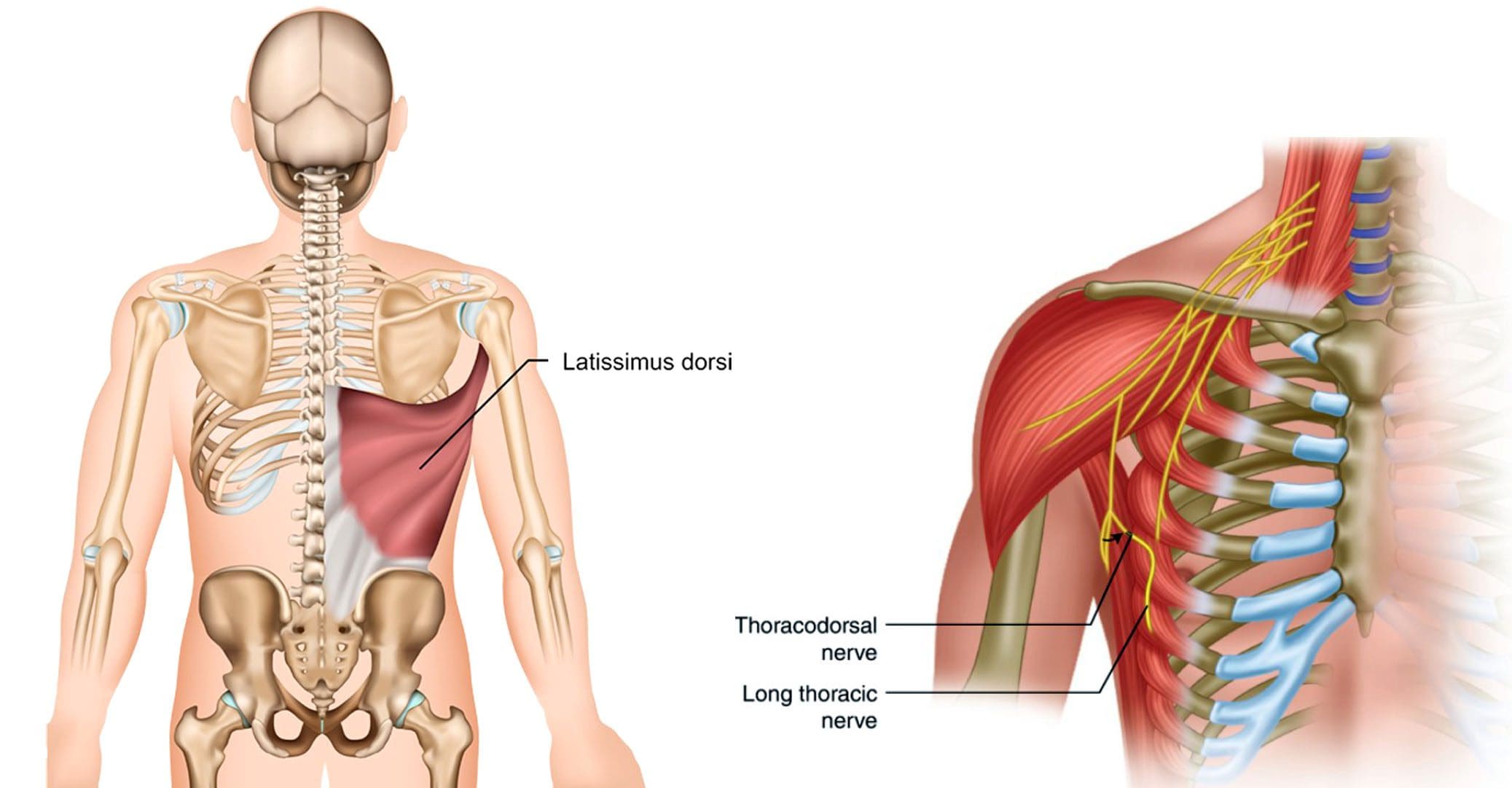
Individuals experiencing pain symptoms like shooting, stabbing, or electrical sensations to the latissimus dorsi of the upper back could be caused by a nerve injury to the thoracodorsal nerve. Can knowing the anatomy and symptoms help healthcare providers develop an effective treatment plan?
Thoracodorsal Nerve
Also known as the middle subscapular nerve or the long subscapular nerve, it branches out from a part of the brachial plexus and provides motor innervation/function to the latissimus dorsi muscle.
Anatomy
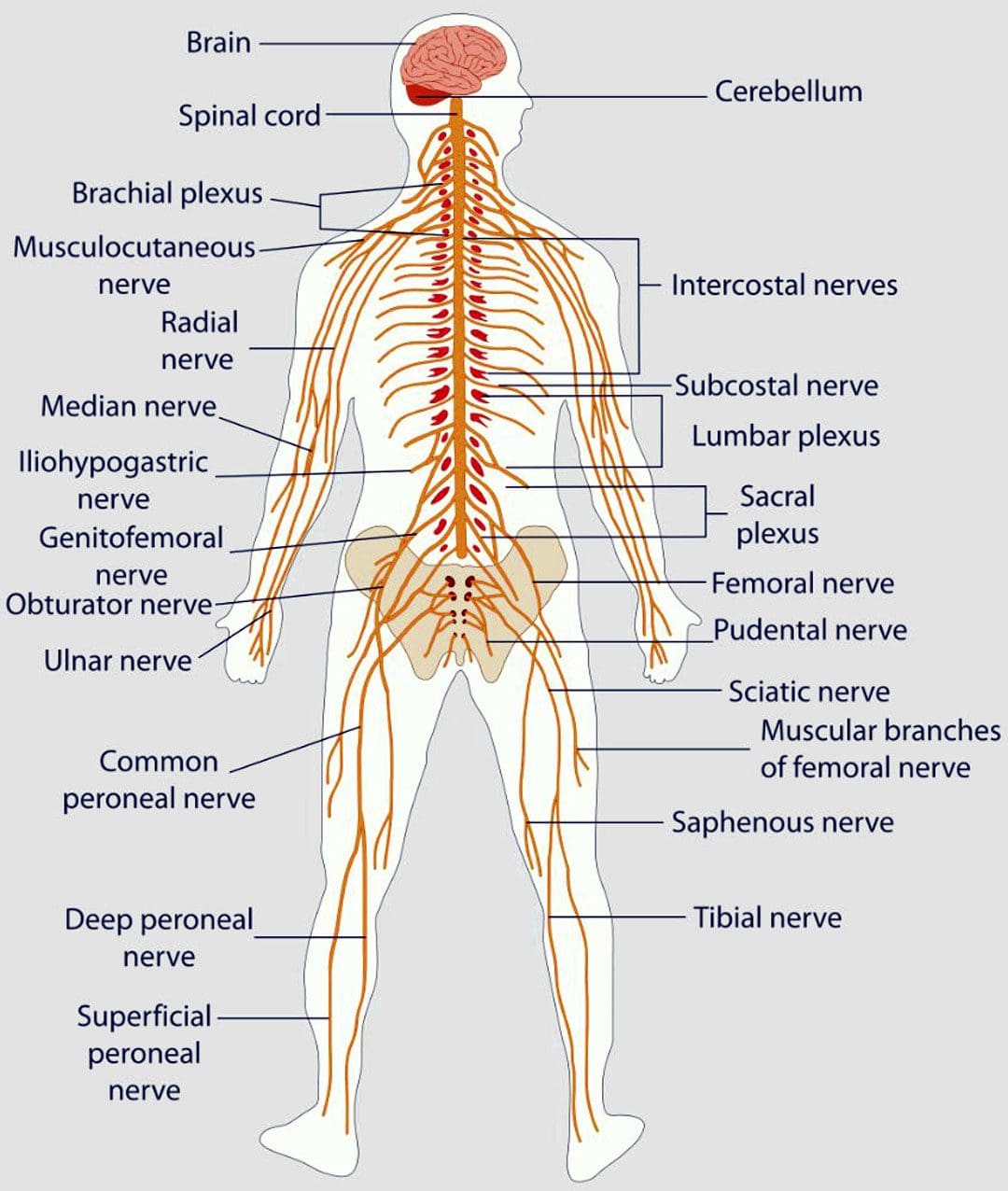
The brachial plexus is a network of nerves that stem from the spinal cord in the neck. The nerves supply most of the sensation and movement of the arms and hands, with one on each side. Its five roots come from the spaces between the fifth through eighth cervical vertebrae and the first thoracic vertebra. From there, they form a larger structure, then divide, re-combine, and divide again to form smaller nerves and nerve structures as they travel down the armpit. Through the neck and chest, the nerves eventually join and form three cords that include:
Lateral cord
Medial cord
Posterior cord
The posterior cord produces major and minor branches that include:
Axillary nerve
Radial nerve
The minor branches include:
Superior subscapular nerve
Inferior subscapular nerve
Thoracodorsal nerve
Structure and Position
The thoracodorsal nerve branches off the posterior cord in the armpit and travels down, following the subscapular artery, to the latissimus dorsi muscle.
It connects to the upper arm, stretches across the back of the armpit, forming the axillary arch, and then expands into a large triangle that wraps around the ribs and the back.
The thoracodorsal nerve lies deep in the latissimus dorsi, and the lower edge typically reaches close to the waist.
Variations
There is a standard location and course of the thoracodorsal nerve, but individual nerves are not the same in everyone.
The nerve typically branches off the posterior cord of the brachial plexus from three different points.
The lats can have a rare anatomical variation known as a Langer’s arch, which is an extra part that connects to muscles or connective tissue of the upper arm beneath the common connecting point.
In individuals with this abnormality, the thoracodorsal nerve supplies function/innervation) to the arch. (Ahmed M. Al Maksoud et al., 2015)
Function
The latissimus dorsi muscle cannot function without the thoracodorsal nerve. The muscle and nerve help:
Stabilize the back.
Pull the body weight up when climbing, swimming, or doing pull-ups.
Assist with breathing by expanding the rib cage during inhalation and contracting when exhaling. (Encyclopaedia Britannica. 2023)
Rotate the arm inward.
Pull the arm toward the center of the body.
Extend the shoulders by working with the teres major, teres minor, and posterior deltoid muscles.
Bring down the shoulder girdle by arching the spine.
Pain that can be shooting, stabbing, or electrical sensations.
Numbness, tingling.
Weakness and loss of function in the associated muscles and body parts, including wrist and finger drop.
Because of the nerve’s path through the armpit, doctors have to be cautious of the anatomical variants so they don’t inadvertently damage a nerve during breast cancer procedures, including axillary dissection.
The procedure is performed to examine or remove lymph nodes and is used in staging breast cancer and in treatment.
According to a study, 11% of individuals with axillary lymph node dissection suffered damage to the nerve. (Roser Belmonte et al., 2015)
Breast Reconstruction
In breast reconstruction surgery, the lats can be used as a flap over the implant.
Depending on the circumstances, the thoracodorsal nerve can be left intact or severed.
There is some evidence that leaving the nerve intact can cause the muscle to contract and dislocate the implant.
An intact thoracodorsal nerve may also cause atrophy of the muscle, which can lead to shoulder and arm weakness.
Graft Uses
A portion of the thoracodorsal nerve is commonly used in nerve graft reconstruction to restore function after injury, which includes the following:
Musculocutaneous nerve
Accessory nerve
Axillary nerve
The nerve can also be used to restore nerve function to the triceps muscle in the arm.
Rehabilitation
If the thoracodorsal nerve is injured or damaged, treatments can include:
Braces or splints.
Physical therapy to improve range of motion, flexibility, and muscle strength.
If there is compression, surgery may be required to alleviate the pressure.
Exploring Integrative Medicine
References
Chu B, Bordoni B. Anatomy, Thorax, Thoracodorsal Nerves. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK539761/
Al Maksoud, A. M., Barsoum, A. K., & Moneer, M. M. (2015). Langer’s arch: a rare anomaly affects axillary lymphadenectomy. Journal of surgical case reports, 2015(12), rjv159. doi.org/10.1093/jscr/rjv159
Belmonte, R., Monleon, S., Bofill, N., Alvarado, M. L., Espadaler, J., & Royo, I. (2015). Long thoracic nerve injury in breast cancer patients treated with axillary lymph node dissection. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer, 23(1), 169–175. doi.org/10.1007/s00520-014-2338-5
Kwon, S. T., Chang, H., & Oh, M. (2011). Anatomic basis of interfascicular nerve splitting of innervated partial latissimus dorsi muscle flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS, 64(5), e109–e114. doi.org/10.1016/j.bjps.2010.12.008
Can individuals with sensory nerve dysfunction incorporate nonsurgical decompression to restore sensory-mobility function to their bodies?
Introduction
The spinal column in the musculoskeletal system comprises bones, joints, and nerves that work together with various muscles and tissues to ensure that the spinal cord is protected. The spinal cord is part of the central nervous system where the nerve roots are spread out to the upper and lower body parts that supply sensory-motor functions. This allows the body to move and function without pain or discomfort. However, when the body and spine ages or when a person is dealing with injuries, the nerve roots can become irritated and cause weird sensations like numbness or tingling, often correlating with body pain. This can cause a socio-economic burden on many individuals and, if not treated right away, can lead to chronic pain. To that point, it can lead to many individuals dealing with body extremity pain associated with sensory nerve dysfunction. This causes many individuals dealing with musculoskeletal disorders to start looking for treatment. Today’s article examines how nerve dysfunction affects the extremities and how nonsurgical decompression can help reduce nerve dysfunction to allow mobility back to the upper and lower limbs. We speak with certified medical providers who incorporate our patients’ information to provide nonsurgical solutions like decompression to help individuals with nerve dysfunction. We also inform patients how nonsurgical decompression can restore mobility-sensory to the upper and lower extremities. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the sensory nerve dysfunction. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
How Nerve Dysfunction Affects The Extremities
Do you experience tingling or numb sensations in your hands or feet that don’t want to go away? Do you feel pain in different back portions that can only be relieved through stretching or resting? Or does it hurt to walk for long distances that you feel like you need to rest constantly? Many pain-like scenarios are associated with sensory nerve dysfunction that can affect the upper and lower extremities. When many individuals experience sensory nerve dysfunction and deal with weird sensations in their extremities, many think it is due to musculoskeletal pain in their neck, shoulders, or back. This is only part of the issue, as many environmental factors can be associated with sensory nerve pain, as the nerve roots are being compressed and agitated, causing sensory nerve dysfunction in the extremities. Since the nerve roots are spread out from the spinal cord, the brain sends the neuron information to the nerve roots to allow sensory-mobility function in the upper and lower extremities. This allows the body to be mobile without discomfort or pain and functional through daily activities. However, when many individuals start to do repetitive motions that cause the spinal disc to be compressed constantly, it can lead to potential disc herniation and musculoskeletal disorders. Since numerous nerve roots are spread to the different extremities, when the main nerve roots are aggravated, it can send pain signals to each extremity. Hence, many people are dealing with nerve entrapment that leads to lower back, buttock, and leg pain that can affect their daily routine. (Karl et al., 2022) At the same time, many people with sciatica are dealing with sensory nerve dysfunction that affects their walking ability. With sciatica, it can be associated with spinal disc pathology and causes many individuals to seek treatment. (Bush et al., 1992)
Sciatica Secrets Revealed-Video
When it comes to looking for treatment to reduce sensory nerve dysfunction, many individuals will opt for nonsurgical solutions to minimize the pain-like symptoms and reduce the pain signals that are causing the upper and lower extremities to suffer. Nonsurgical treatment solutions like decompression can help restore sensory nerve function through gentle traction by causing the spinal disc to lay off the aggravated nerve root and start the body’s natural healing process. At the same time, it helps reduce musculoskeletal disorders from returning. The video above shows how sciatica associated with sensory nerve dysfunction can be decreased through nonsurgical treatments to allow the body’s extremities to feel better.
Nonsurgical treatments can help reduce low back pain associated with sensory nerve dysfunction to restore sensory-motor function to the upper and lower extremities. Many individuals who incorporate nonsurgical treatments like decompression as part of their health and wellness routine can see improvement after consecutive treatment. (Chou et al., 2007) Since many healthcare practitioners incorporate nonsurgical treatments like decompression into their practices, there has been quite an improvement in pain management. (Bronfort et al., 2008)
When many individuals start to use nonsurgical decompression for sensory nerve dysfunction, many will see improvement in their pain, mobility, and activities of their daily living. (Gose et al., 1998). What spinal decompression does for the nerve roots is that it helps the affected disc that is aggravating the nerve root, pulls the disc back to its original position, and rehydrates it. (Ramos & Martin, 1994) When many individuals start thinking about their health and wellness, nonsurgical treatments can be effective for them due to their affordable cost and how they can be combined with other therapies to manage better the pain associated with nerve dysfunction affecting their body extremities.
References
Bronfort, G., Haas, M., Evans, R., Kawchuk, G., & Dagenais, S. (2008). Evidence-informed management of chronic low back pain with spinal manipulation and mobilization. Spine J, 8(1), 213-225. doi.org/10.1016/j.spinee.2007.10.023
Bush, K., Cowan, N., Katz, D. E., & Gishen, P. (1992). The natural history of sciatica associated with disc pathology. A prospective study with clinical and independent radiologic follow-up. Spine (Phila Pa 1976), 17(10), 1205-1212. doi.org/10.1097/00007632-199210000-00013
Chou, R., Huffman, L. H., American Pain, S., & American College of, P. (2007). Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med, 147(7), 492-504. doi.org/10.7326/0003-4819-147-7-200710020-00007
Gose, E. E., Naguszewski, W. K., & Naguszewski, R. K. (1998). Vertebral axial decompression therapy for pain associated with herniated or degenerated discs or facet syndrome: an outcome study. Neurol Res, 20(3), 186-190. doi.org/10.1080/01616412.1998.11740504
Karl, H. W., Helm, S., & Trescot, A. M. (2022). Superior and Middle Cluneal Nerve Entrapment: A Cause of Low Back and Radicular Pain. Pain Physician, 25(4), E503-E521. www.ncbi.nlm.nih.gov/pubmed/35793175
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. doi.org/10.3171/jns.1994.81.3.0350
For individuals dealing with chronic pain conditions can having a better understanding of pain management specialists help in developing effective multidisciplinary treatment plans?
Pain Management Specialists
Pain management is a growing medical specialty that takes a multi-disciplinary approach to treating all types of pain. It is a branch of medicine that applies scientifically proven techniques and methods to relieve, reduce, and manage pain symptoms and sensations. Pain management specialists evaluate, rehabilitate, and treat a spectrum of conditions, including neuropathic pain, sciatica, postoperative pain, chronic pain conditions, and more. Many primary healthcare providers refer their patients to pain management specialists if pain symptoms are ongoing or significant in their manifestation.
Specialists
Healthcare providers specializing in pain management recognize the complex nature of pain and approach the problem from all directions. Treatment at a pain clinic is patient-centric but depends on the clinic’s available resources. Currently, there are no set standards for the types of disciplines needed, another reason treatment options vary from clinic to clinic. Experts say that a facility should offer patients:
A coordinating practitioner specializing in pain management and consulting specialists on the patient’s behalf.
Other specialties represented in pain management are anesthesiology, neurosurgery, and internal medicine. A coordinating healthcare provider may refer an individual for services from:
A healthcare provider should have completed additional training and credentialing in pain medicine and be an MD with board certification in at least one of the following (American Board of Medical Specialties. 2023)
Anesthesiology
Physical rehabilitation
Psychiatry
Neurology
A pain management physician should also have their practice limited to the specialty they hold the certification.
Management Goals
The field of pain management treats all types of pain as a disease. Chronic, such as headaches; acute, from surgery, and more. This allows for applying science and the latest medical advances to pain relief. There are now many modalities, including:
Medication
Interventional pain management techniques – nerve blocks, spinal cord stimulators, and similar treatments.
Physical therapy
Alternative medicine
The objective is to minimize and make symptoms manageable.
Individuals determined that surgery does not benefit their condition.
A better understanding of pain syndromes by communities and insurance companies and increased pain studies will help increase insurance coverage for treatments and technology to improve interventional outcomes.
Nalamachu S. (2013). An overview of pain management: the clinical efficacy and value of treatment. The American journal of managed care, 19(14 Suppl), s261–s266.
American Society of Interventional Pain Physicians. (2023). Pain Physician.
Individuals feeling tingling or pins and needles sensations that overtake the arms or legs could be experiencing paresthesia, which occurs when a nerve has been compressed or damaged. Can knowing the symptoms and causes help in diagnosis and treatment?
Paresthesia Body Sensations
The numbness or tingling feeling when an arm, leg, or foot has fallen asleep is not so much about blood circulation but nerve function.
Paresthesia is an abnormal sensation felt in the body due to the compression or irritation of nerves.
It can be a mechanical cause like a compressed/pinched nerve.
Or it may be due to a medical condition, injury, or illness.
The symptoms typically last for 30 minutes or less.
Shaking the affected limb often relieves the sensations.
Paresthesia usually affects only one arm or leg at a time.
However, both arms and legs can be affected, depending on the cause.
Consult a healthcare provider if the symptoms last for more than 30 minutes. Treatment may be required if paresthesia body sensations are brought on by a serious underlying cause.
Causes
Sitting with incorrect and unhealthy postures can compress a nerve and generate symptoms. However, some causes are more concerning and can include:
If the symptoms don’t go away after 30 minutes or keep returning for unknown reasons, call a healthcare provider to find out what is causing the abnormal sensations. A worsening case should be monitored by a healthcare provider.
Peripheral neuropathy caused by diabetes usually begins with a feeling of paresthesia in the foot/feet and can worsen and lead to other complications.
A healthcare provider will work with the individual to understand the symptoms and perform the appropriate diagnostic tests to determine the cause. A healthcare provider will choose the tests based on a physical examination. Common diagnostic procedures include: (Merck Manual Professional Version. 2022)
Magnetic resonance imaging – MRI of the spine, brain, or extremities.
X-ray to rule out bone abnormalities, like a fracture.
Blood tests.
Electromyography – EMG studies.
Nerve conduction velocity – NCV test.
If paresthesia is accompanied by back or neck pain, a healthcare provider may suspect a compressed/pinched spinal nerve.
If the individual has a history of diabetes that is poorly controlled, they may suspect peripheral neuropathy.
Treatment
Treatment for paresthesia depends on the diagnosis. A healthcare provider can help determine the best course of action for the specific condition.
Nervous System
If symptoms are triggered by a central nervous condition like MS, individuals will work closely with their healthcare provider to get the appropriate treatment.
If paresthesia is caused by compression of a spinal nerve, like sciatica, individuals may be referred to a chiropractor and physical therapy team to release the nerve and pressure. (Julie M. Fritz, et al., 2021)
A physical therapist may prescribe spinal exercises to relieve compression of the nerve and restore normal sensations and motion.
Strengthening exercises to restore flexibility and mobility may be prescribed if weakness presents along with paresthesia body sensations.
Herniated Disc
If a herniated disc is causing the abnormal sensations, and there has been no improvement with conservative measures, a healthcare provider may suggest surgery to relieve pressure on the nerve/s. (American Association of Neurological Surgeons. 2023)
In surgical procedures like a laminectomy or discectomy, the objective is to restore nerve function.
Post-surgery, individuals may be recommended to a physical therapist to help regain mobility.
National Institute of Neurological Disorders and Stroke. (2023) Paresthesia.
American Association of Neurological Surgeons. (2023) Herniated disc.
National Institute of Diabetes and Digestive and Kidney Diseases. (2018) Peripheral neuropathy.
Merck Manual Professional Version. (2022) Numbness.
Razazian, N., Yavari, Z., Farnia, V., Azizi, A., Kordavani, L., Bahmani, D. S., Holsboer-Trachsler, E., & Brand, S. (2016). Exercising Impacts on Fatigue, Depression, and Paresthesia in Female Patients with Multiple Sclerosis. Medicine and science in sports and exercise, 48(5), 796–803. doi.org/10.1249/MSS.0000000000000834
Fritz, J. M., Lane, E., McFadden, M., Brennan, G., Magel, J. S., Thackeray, A., Minick, K., Meier, W., & Greene, T. (2021). Physical Therapy Referral From Primary Care for Acute Back Pain With Sciatica : A Randomized Controlled Trial. Annals of internal medicine, 174(1), 8–17. doi.org/10.7326/M20-4187
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine